110 Poliomyelitis
Poliomyelitis is an acute disease caused by inflammation and destruction of motor neurons after infection by a poliovirus. Sensory functions are not affected. Although frequently asymptomatic, the infection may cause fever and a number of other general symptoms, described as abortive polio or minor illness.
Occasionally, however, these prodromal symptoms are followed a few days later by infection of the central nervous system (CNS) and fever, with meningitis, or paresis (weakness) or paralysis of one or more muscles. Many patients recover use of the muscle or some muscles affected in the following months, although some have permanent paralysis or paresis. When the muscles of respiration are affected, death may follow.Other enteroviruses of the ECHO (Enteric Cyto- pathic Human Orphan virus) and Coxsackie groups may also cause meningitis and paresis, or temporary paralysis. In the past, cases of abortive polio and those with paralysis who later recovered were often included in statistics as polio cases. Today, only cases with paralysis or paresis after 3 months are recorded as paralytic polio.
Poliomyelitis was known by several names until the 1870s, when it became known as acute anterior poliomyelitis. Among them was Heine-Medin disease (after two early researchers, Jacob von Heine and Karl Oscar Medin) and infantile paralysis because it affected mainly young children. As more adults and older children were affected, poliomyelitis - inflammation of the gray marrow - became the name of choice and is often shortened to polio.
Etiology and Immunology
There are three immunologic types of poliovirus, with strain differences in each, and there may be minor cross-reactions between types 1 and 2. Within each type there is a wide range of ability to cause paralysis, from the highly virulent type 1 Mahoney strain to avirulent wild and vaccine strains.
Wild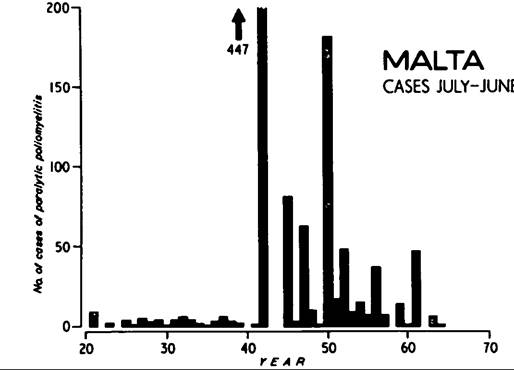
Figure VIII.110.1. Cases of paralytic poliomyelitis in Malta, 1920-64. Epidemics always occurred in the winter, with no cases in June to July even in other years; the cases are counted from July of one year to June of the next to emphasize the epidemics. Cases are those notified except for 1942, when late-diagnosed cases are included. In the late 1950s and early 1960s, inactivated poliovirus vaccine (IPV) was given to groups already mostly immune. In 1964 oral poliovirus vaccine (OPV) was given to all age groups and, from then on, to young babies and children.
strains may cause only a few cases of paralysis while immunizing other children. The introduction of a new virulent strain, however, may cause an epidemic, as in Malta in 1942 (Figure VΠI.110.1). Strains differ widely in their transmissibility: In Malta, the pattern of cases among children in villages, among British servicemen, and in the next epidemic suggests that everyone in the island was rapidly infected. There are many other examples, however, of small epidemics without further cases in the region. The new technique of genomic sequencing has shown that small epidemics, many hundreds of miles apart, may be caused by viruses that are very similar.
The virus spreads from person to person via the fecal-oral route, although a few epidemics may have been caused by contaminated milk. Ingested virus replicates in the gut and associated lymphoid tissue. After 2 to 3 days, there is viremia lasting until about day nine, when the virus is neutralized by serum antibody. The level of viremia correlates with virulence; there is little or no viremia with avirulent strains. Animal experiments suggest that the level of antibody that protects is below the threshold of detection.
Exposure to virus leads to lifelong immunity to viruses of the same type. Although people who are immune have some gut immunity, they may still be infected but they have no viremia and shed less virus for a shorter time.
Humans are the only natural host and reservoir, although other primates may be infected experimentally or accidentally.Since 1910 it seemed that immunization might be feasible. The first attempts in 1935 ended with cases and deaths attributed to the vaccines. Many vaccines were made for experimental use only, but a vaccine for humans was not possible until the virus could be grown in quantity outside the central nervous system of monkeys, the number of antigenic types could be established, and cheap methods of titrating virus and antibody could be developed. J. F. Enders, T. H. Weller, and F. C. Robbins grew poliovirus in human tissue culture in late 1948 and solved all three problems. In 1951 Hilary Koprowski fed an attenuated virus to 20 adults.
In 1953 Jonas Salk injected an inactivated vaccine (IPV) into over 100 children, and in the following year the vaccine was given to 400,000 children in an elaborate field trial involving 1.8 million children. The effort was successful, but a slightly different vaccine was finally licensed. Vaccine from at least one manufacturer — Cutter Laboratories — contained live virions, and there were about 250 resulting cases in what was called the “Cutter incident” of 1955. Manufacture and safety testing of the Salk vaccine were tightened but at the cost of reduced antigenicity. In the 1980s, a purified and more antigenic IPV was produced that required two doses instead of three to produce lasting immunity.
Two early attenuated oral poliovaccines (OPV), the Koprowski and Cox-Lederle vaccines, had been given trials in several countries but were abandoned. Use of the Cox-Lederle vaccine in West Berlin in the spring of 1960 was followed by a few cases that might have been vaccine-associated. On the other hand, inflammation in a muscle, caused by an injection, can greatly increase the chance of paralysis, and it may be that a drug such as thalidomide, which causes peripheral neuritis, might act in the same way, although without the localization that is the hallmark of provocation polio.
Thalidomide, which was in use in 1960, caused peripheral neuritis, and analysis of the cases is consistent with the theory that thalidomide made those taking it more susceptible to CNS invasion by the vaccine virus.In the 1950s A. B. Sabin produced an oral polio vaccine (OPV), which has been used extensively throughout the world. The advantages of the Sabin vaccine are many: (1) It can be given by nonmedical staff under supervision; (2) it induces gut immunity; (3) it is inexpensive; and (4) immunity spreads to others not given the vaccine. Yet there are disadvantages: (1) Three separate doses are required; (2) it is quickly inactivated by heat; and (3) the virus reverts toward virulence and causes some vaccine-associated cases (VAC). Although there is no evidence that it can harm pregnant women, the Sabin vaccine is not given to them. About one child in a million given OPV develops paralysis. Early figures of risk were based on doses, not children, and included large numbers who were already immune and so not at risk. Hypogammaglobulinemic children are at risk from OPV, and a small number (about 2 percent) develop a chronic CNS infection with paralysis. A very small number of contact VAC occur, mainly among mothers of children given OPV The number of such cases depends on the number of people who have not been immunized by vaccine or wild viruses.
Oral polio vaccine has been used very successfully in countries with temperate climates but less so in many warmer developing countries. The problems have been largely due to lack of cold-chain facilities (to prevent heat inactivation) and organization. The most effective method of immunization is the once or twice a year “polio day” pulse program. Distribution of the vaccine is made a few days before immunization to local immunization posts throughout the whole country, reducing the problems presented by the cold chain. On the day of immunization, which is heavily advertised in the media, all children 2 years and younger who are present are given OPV The flood of virus shed by vaccinees then vaccinates any who did not receive OPV and displaces circulating wild virus.
Inactivated polio vaccine is more stable and may be combined with other vaccines such as that of diphtheria—pertussis-tetanus (DPT), thus simplifying immunization schedules and reducing cost. The latest IPV is very safe, highly purified, and antigenic. Although one dose may suffice, at least two doses are recommended.
Epidemiology
In most years it is very difficult to assess epidemics because there may be several polioviruses of different virulence and types circulating. Thus the extent of the circulation of the virulent viruses will not be known and the cases will not necessarily correspond to the geographic boundaries used for reporting. Moreover, because viruses change their virulence, the number of nonimmunes will be unknown. Surveys of immune status and examination of feces for virus are expensive and time-consuming, and sam-
pie only a tiny fraction of a given population. Thus our epidemiological knowledge of the disease is very dependent on virgin soil epidemics in islands and isolated communities with definite boundaries that contain many nonimmunes.
After an epidemic in 1919, polio was made a notifiable disease in Malta. About three cases were reported each year (Figure VIII.110.1) until 1942, when almost 3 percent of children under 3 years of age were stricken. Other epidemics followed at intervals of 2 or 3 years. Some of these epidemics were probably caused by the importation of virulent viruses from Egypt by returning Maltese in 1919, 1945, and 1947 and by the arrival by overnight flight of about 250 RAF men in 1942. Nearly all the Maltese cases were children under 5 years of age.
Prior to the 1930s, most polio cases occurred in young children, except in small isolated communities where older children, adolescents, and even adults were sometimes affected. Beginning in the 1930s, however, there was a shift to older children and adolescents, first in Scandinavia and the United States, and then in Europe.
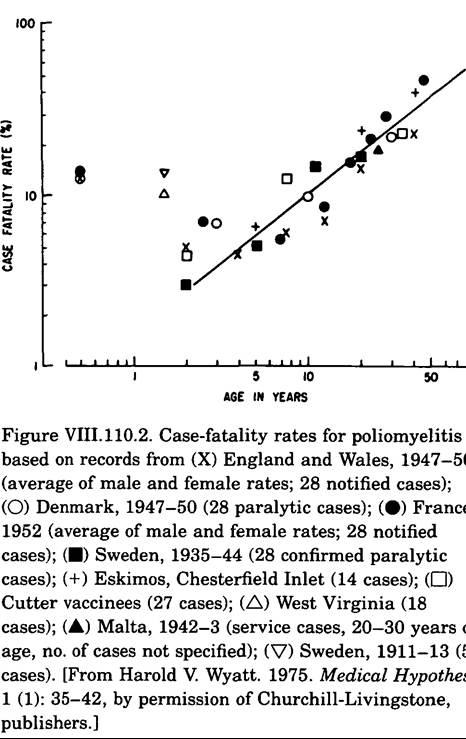
The older children suffered less paralysis, and, as Figure VIILl 10.2 shows, the case-fatality rate was low. By contrast, young adults had paralysis and case-fatality rates like those of small children. In many severe epidemics, the case-rate for 2-year-olds has been about 2 percent with increasing rates up to about 10 years of age, when the rate stabilizes at 25 percent. In a virgin soil epidemic among an Eskimo population in 1948, 2 out of 53 children and 25 percent of adolescents and adults were paralyzed.Incidence in monozygotic and dizygotic twins suggests genetic susceptibility, and there are families who have had many cases over several generations. Yet, the overall level of familial incidence is low, and genetic susceptibility has been largely discounted. On the other hand, the changes in paralysis and case-fatality rates at about 3 years of age can be explained if two groups are genetically susceptible - the 2 percent of the population who are homozygotes and the 24 percent who are heterozygotes. This model suggests that genetic susceptibility is a maturation process, with about half the homozygotes becoming phenotypically susceptible at 1 year of age and all at 2 years. Heterozygotes would mature more slowly, reaching 24 percent at about 10 years.
Early epidemiological surveys often included all cases whether there was residual paralysis or not, and cases of abortive polio were also frequently included, although diagnosis in these cases is difficult and uncertain. From the late 1930s, it became increasingly common to restrict inclusion in the statistics to those with paralysis, and later only to those with residual paralysis. In countries where there is universal immunization and very few cases, each suspected case is investigated. A positive virus isolation or a rise in antibody titer between acute and convalescent sera is evidence of poliovirus involvement. Polioviruses are tested for affinity to vaccine and wild strains.
Distribution and Incidence
At all ages, there are more male than female cases. However, pregnant females have a higher incidence of poliomyelitis than nonpregnant females of the same age. Attempts to explain these differences have been unsuccessful. The case-fatality rates of males and females are similar. Studies of many hundred pregnant women with polio showed no increase in miscarriages, and there were no affected births. Moreover, 48 stillborn or aborted fetuses showed no signs of polio. A few fetuses have been examined for virus, which was isolated from many organs. The one stillborn fetus tested was positive for virus in the CNS (Wyatt 1979).
Yet when the mother had suffered paralysis between 7 days before and 10 days after birth, 40 percent of the babies suffered concurrent paralysis, with a 56 percent case-fatality rate. By contrast, babies bom of mothers who had experienced paralysis earlier in the pregnancy (nonconcurrent) had a less than 0.01 percent chance of polio in the month after birth and only a 10 percent case-fatality rate. The few babies bom by Caesarian section of mothers who contracted polio just before birth were not affected. Babies with paralysis 0 to 10 days after birth had a very short incubation time - 6 days - as compared with 12 days for concurrent cases in babies with paralysis 11 to 28 days after birth.
When a nonimmune person who is infected with a virulent poliovirus receives an injection of an inflammatory substance into a muscle, the chance of paralysis occurring 7 to 18 days later is much increased. In many cases, the muscle receiving the injection is the first paralyzed and the extent and severity of paralysis may also be increased. The phenomenon, called provocation, was recognized in 1950, when mass immunization with diphtheria-pertussis-tetanus vaccine (DPT) began. Risk of provocation was much reduced by giving DPT in winter when circulation of poliovirus was minimal. Sterile saline and human gammaglobulin did not provoke. Provocation had first been described, but not named, in 1914 when nearly a quarter of 22 babies with congenital syphilis were paralyzed with polio after treatment with multiple injections of Salvarsan. Further epidemics with 25 percent case-rates were noted in Rome between 1936 and 1947 among similar children given multiple injections OfSalvarsan (arsphenamine) and, later, penicillin. Similarly, nonepidemic polio among children with congenital syphilis in Rome and London showed case-rates up to 25 times the rate in ordinary children, and simliar rates were seen in epidemics in the South Pacific in 1932 and 1951.
The degree of provocation increases with the ability to produce inflammation: Thus vaccines with adjuvants are more provocative than those without. Single injections may increase the risk up to 8 times, whereas multiple injections may increase the risk 25 times.
Injection of live poliovirus, as in the Cutter incident, may cause paralysis with features similar to provocation polio but with a shorter incubation. Toxocara infection increases the risk of polio: The dead larvae in the muscles may act as centers of provocation.
Tonsillectomy - but probably not tonsillotomy - increases the risk of paralysis and especially the risk
Table VIII.110.1. Comparison Ofparalysis of lower limbs in temperate and developing countries
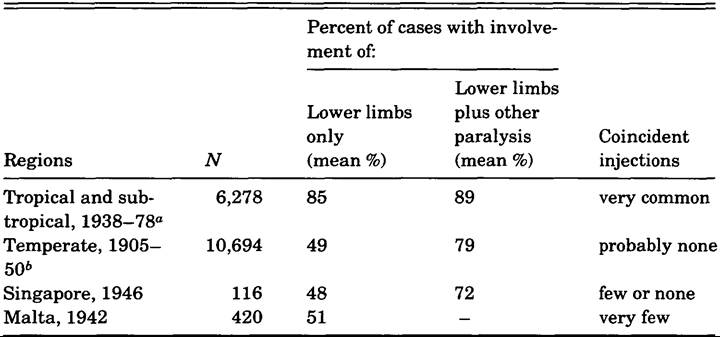
“Based on 12 papers: from Sri Lanka (1 paper), Madagascar (1), India (5), Nigeria (2), Congo (1), Cameroun (1), and Bahrain and Kuwait (1).
6Based on 9 papers: from the United States (4), the United Kingdom (2), Sweden (1), Denmark (1), and Germany (1).
of bulbar polio. The increased risk not only is immediate but also persists for 5 or more years. The incubation time immediately after the operation is from 7 to 17 days - the same as for ordinary polio - which implies that entry of the virus does not occur directly in the oropharynx but only after viremia.
As immunity to polio is mediated by antibody, all hypogammaglobulinemics should be particularly susceptible. Before antibiotics, most of these children probably died Ofbacterial infections, but from 1950 to 1960, of 154 children and adults with inherited or acquired hypogammaglobulinemia, only 8 developed polio - about the number expected on the genetic model. Only about 2 percent of Iiypogammaglobuli- nemic children — about 10 percent of VAC children - develop polio after OPV has been given. The incubation is longer than 28 days; there is a high mortality after a long chronic illness, with abnormal lesions in the CNS and no reversion to virulence of the virus. Hypogammaglobulinemics are about 10,000 times more likely than other children to develop polio after the oral administration of polio vaccine.
Clinical Manifestations and Pathology
During the prodromal stage, there is viremia, and replication of virus occurs in the muscles. There may be muscle pains as well as fever. About 25 percent of those infected may show signs of abortive polio. There are two theories as to how virus reaches the CNS. The first suggests that virus crosses the bloodbrain barrier (BBB) and travels along neuronal pathways in the CNS. However, David Bodian showed that virus traveled up the sciatic nerve at 2.4 mm per hour. Postmortems reveal that lesions in the CNS can be discrete and separate, suggesting that virus enters at numerous endplate junctions of motor neurons in the muscles and reaches the CNS at many different places. The time taken to reach the CNS from any muscle depends on the length of the nerve to be traveled, during which time the virus would be shielded from antibody. Virus could enter a nerve at any time from about the second to the ninth day. Virus entering from a foot muscle on the ninth day in a tall adult would reach the CNS about 18 days later. This model would account for the incubation of about 3 to 28 days. As viremia ends about the ninth day, the BBB model requires the virus to be 18 days in the CNS before producing symptoms.
Leg muscles are more often affected than arms, as indicated in Table VIII.110.1. In general, the larger the muscle the greater the chance of paralysis, and the smaller the muscle the greater the chance of paresis. Muscles are not affected at random. The neurons serving them lie in adjacent and overlapping bundles in the CNS: Damage in one bundle will often spill over into an adjacent bundle, so there is a high probability that both muscles will be affected.
Up to 60 percent of the neurons serving a muscle may be destroyed before there is a loss of function, and thus patients who have had nonparalytic CNS infection may still have suffered considerable damage. In one such patient who was examined after death from an unrelated accident, there were a number of separate regions of damage. Many survivors
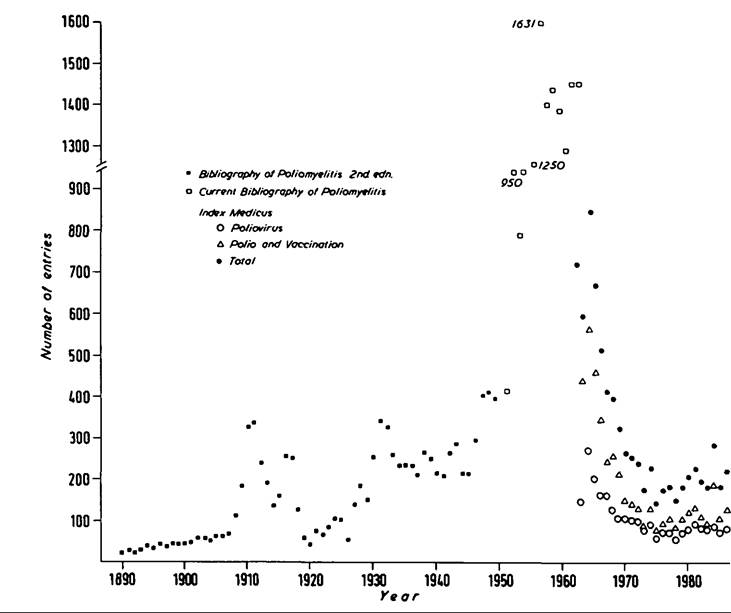
Figure VIII.110.3. Numbers of publications about polio by year, 1890 to 1986. The figures are not entirely comparable: The Current Bibliography of Poliomyelitis includes some papers about other viruses; Index Medicus puts the entry for a single paper in more than one section, so that the number of papers is overestimated by perhaps 5 percent. Entries in the Bibliography of Infantile Paralysis are listed by year of publication, whereas other bibliographies list entries by year of appearance in the secondary serial (e.g., 6 months later). The effects of world wars, slumps, large epidemics, and notable research findings are apparent (see J. R. Paul 1971). The peak of papers in 1984 is due to an international conference held in 1983.
are suffering late effects of polio (LEP) more than 30 years later. Previously unaffected muscles become weak; already affected muscles become weaker; and in addition, generalized weakness and fatigue occur. The muscles most commonly affected are those that recovered well from the initial attack and have been used strenuously ever since. There is continual loss of motor neurons with age, and LEP may be the effect of normal aging superimposed on previous loss through polio.
In the acute stage, there is massive proliferation of lymphocytes in lymph nodes, and the picture in the CNS resembles a host-versus-graft reaction. Infected neurons are destroyed, although the inflammation does not correspond with the location of virus. Delayed hypersensitivity to poliovirus does not occur, even after many injections of vaccine. Moreover, the short response time suggests that the lymphocyte proliferation is a secondary response. Sabin showed that some adults gave a skin response to primate gray matter. One explanation could be that infected neurons are damaged with loss of function, but that more damage is caused by lymphocytes sensitized to motor neuron antigen. The proportion of damage caused by virus and lymphocytes may depend on the presence of antibody. In animal experiments, Bodian observed that 75 percent of infected neurons recover.
Second attacks by a virus of a different type presumably should occur; yet only 44 have been reported - far less than one might expect. This and animal experiments, however, suggest that second attacks are not blocked by antibody against poliovirus. Some Iiypogaminaglobulinemics suffer a chronic infection, and animal experiments show that coincident infections with other enteroviruses can be synergistic.
History and Geography
Polio may be as old as humankind, but there are very few early indicators of the disease. An Egyptian stele from about 1400 B.C., now in the Carlsberg Glyptothek, Copenhagen, shows a young priest with a shortened, deformed foot in the typical equinus position of polio. In the 1830s, three small epidemics of the disease were reported from England, the United States, and the island of Saint Helena. In the 1890s and early 1900s, there were more serious epidemics reported in Scandinavia, Massachusetts, and Vermont, and then the great New York epidemic of 1916 occurred with over 9,000 cases in the city itself. Almost all the patients in the New York epidemic were under 5 years of age, and 2 percent of the children aged 2 years were affected. After this, polio cases in the United States fell to a low level, then showed peaks and troughs, and rose again to an annual average of some 40,000 cases from 1951 to 1955. As Figure VIIL 110.3 shows, polio research accompanied these peaks and troughs.
After 1955, with the widespread use of the IPV in the United States, Canada, South Africa, Australia, and some countries in Europe, the number of cases fell dramatically. As not all children were immunized, small epidemics still occurred among the poor living in substandard conditions. But soon almost all the countries in temperate climates were using polio vaccine, and the potency of the vaccine was improved. Nonetheless, by 1960 in the United States in particular, there were doubts that IPV would eliminate polio.
By the end of 1960, however, Sabin OPV, given to more than 115 million people in Russia and Eastern Europe, had almost completely eliminated polio there. Gradually, opinion swung toward the routine use of the OPV instead of IPV, although Scandinavia and Holland continued to use IPV
With these exceptions, beginning in 1961, OPV was increasingly used in countries with the most temperate climate, and the number of polio cases fell to even lower levels, although there were still small epidemics where wild virus struck communities that refused immunization or were not receiving primary health care. In the United States there are now about 10 cases a year, roughly half of which are vaccine-associated in vaccines or their contacts, or in Iiypogammaglobulinemic children.
In Holland, by contrast, there is a large community that rejects immunizations on religious grounds, and thus these people have suffered eight epidemics since 1960. The disease has not, however, spread to the immunized population. The last epidemic, which occurred in 1978, produced IlO cases of which 79 were paralytic (one baby died) and as a result of which the virus was carried to Canada. There were cases in Alberta, British Columbia, and Ontario, from which it was carried to Pennsylvania, and then to Iowa, Wisconsin, and Missouri, and then back to Canada, causing 21 cases and three nonparalytic attacks in North America. Genomic sequencing of virus isolates from this epidemic confirms that the same virus was involved for over 15 months and on two continents and that it may well have come from Turkey originally.
Polio was previously thought to have been of very low incidence in developing countries, although the disease occurred in such diverse and remote places as Saint Helena, isolated Greenland villages, and Nauru in the southern Pacific, which suffered very severe epidemics. Individual cases in undeveloped countries were noted especially among older Europeans, but it was assumed that almost all infants were infected while still protected by maternal antibodies, and that very few developed paralysis. Despite an outbreak among New Zealand troops in Egypt in 1941 and, during the next few years, among British and U.S. servicemen in the Middle and Far East and India, little attention was paid to the disease, the epidemics in Singapore, the Andaman Islands, and Bombay not withstanding.
Early data from developing countries were based on acute admissions to hospitals and, consequently, seriously underestimate the true number of cases. Indeed, even in the mid-1980s, statistics sent to the World Health Organization (WHO) from individual countries may represent only 10 percent of the true number of the cases. In 1977, by way of illustration, in Nigeria more children attended one physiotherapy clinic than the officially notified number of polio cases for that year for the entire country. A truer estimate of cases can be made by lameness surveys of children in schools supplemented by searches of villages for children so disabled that they do not attend school. Unfortunately, such investigations are always out of date, and do not include those who died of polio. It seems likely that the deaths among girls with polio may be quite high in communities where girls are not as highly regarded as boys.
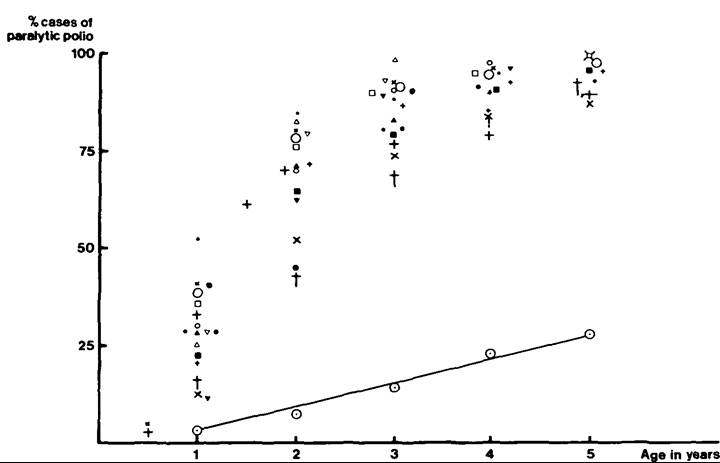
Moreover, case-fatality rates for polio in developing countries are usually based on admission to hospitals and may therefore grossly distort those rates, as only the more serious cases reach those hospitals. Reporting polio cases as an incidence per 100,000 population can also be misleading, as the proportion of children in the population can differ considerably from country to country. The prevalence, based on the total number of cases by the age of 5 years (Figure VIII.110.4), is a better statistic for developing countries.
Even when data on all hospital cases are collected in developing countries, only about half of the cases are found. Up to 10 percent of these cases occur in babies under 6 months, although few studies are this specific (Figure VIII.110.4). Because they will have already had many infections, adults can be expected to have a high level of protective antibodies which mothers should pass on to their babies. Nonetheless, despite repeated infections, pregnant women may still have very low levels of antibodies, and consequently, about 20 to 40 percent of all polio cases occur before the first birthday. For immunization to be effective, all children must be immune by 6 months of age. As Figure VIII.110.4 indicates, giving vaccine to individual children over 1 year is wasteful, and resources should be targeted for the youngest age possible.
Figure VIIL 110.4. Age of onset of cases of poliomyelitis in developing countries, compared with Miami, Florida, United States, 1948-9 (lower points and line). Remaining symbols represent data from samples: Africa (11), India (4), Malta (1), and Singapore (1). (Author’s compilation.)
OPV can be given at birth but is more usually given at intervals some time after. The WHO has set up the Expanded Programme on Immunization (EPI), and Rotary International, Save the Children, and UNICEF are also involved in immunization projects. Thus, by June 1987, WHO estimated that 45 percent of children under 1 year in developing countries (excluding China) had received three doses of vaccine.
Very promising programs are underway in South America; and Argentina, Brazil, Chile, Costa Rica, Cuba, Nicaragua, and Paraguay have programs that reach more than 80 percent of their children below 1 year of age.
In Central Africa, by contrast, few countries achieve a 50 percent immunization rate of children under 1 year of age. Similarly, India, with 22 million children bom each year, immunizes less than half, and many lameness surveys show a rising prevalence among older children in the 5- to 10-year age group, despite increased use of vaccine during the period. Indeed, in India, surveys of all kinds since 1945 have revealed a steady increase in prevalence. This increase may reflect better reporting and investigation or could be due to the widespread use of Unsterile syringes and injections causing provocation polio.
The pattern of muscle paralysis in children in Nigeria is consistent with provocation after injections in the two large muscles. Many children with polio have a history of injections in the paralyzed muscles.
H. V. Wyatt
Bibliography
Bodian, David. 1976. Poliomyelitis and the sources of useful knowledge. Johns Hopkins Medical Journal 138: 130-6.
Enders, John Franklin. 1949. Cultivation of the Lansing strain of poliomyelitis virus in cultures of various human embryonic tissues. Science 109: 85—7.
Flexner, Simon, and Paul A. Lewis. 1910. Experimental poliomyelitis in monkeys: Active immunization and passive serum protection. Journal of the American Medical Association 54:1780—2.
Hedley, O. F. 1940. Public Health Reports 55: 1647—91.
Koprowski, Hilary, et al. 1952. Immune responses in human volunteers upon oral administration of a rodent- adapted strain Ofpoliomyelitis virus. American Journal of Hygiene 55: 108-26.
Lambert, A. 1920. Acute rheumatic fever. Journal of the American Medical Association 74: 993—5.
Paul, John R. 1971. A history ofpoliomyelitis. New Haven. Sabin, Albert B. 1955. Characteristics and genetic potentialities of experimentally produced and naturally occurring variants of poliomyelitis virus. Annals of the New York Academy OfSciences 61: 924—38.
Sabin, Albert B., and Peter K. Olitsky. 1936. Cultivation of poliomyelitis virus in vitro in human embryonic nervous tissue. Proceedings of the Society for Experimental Biology and Medicine 34: 357—9.
Salk, Jonas E., et al. 1953. Studies in human subjects on active immunization against poliomyelitis. I. A preliminary report of experiments in progress. Journal of the American Medical Association 151: 1081-98.
Underwood, Michael. 1789. Treatise on the diseases of children. London.
Wickman, Ivan. 1913. Acute poliomyelitis. Nervous and mental diseases monograph series No. 16. New York.
World Health Organization. 1955. Poliomyelitis. Monograph series No. 26. Geneva.
Wyatt, Harold V. 1973a. Hypogammaglobulinemia and poliomyelitis. Journal OfInfectious Diseases 128: 802-6.
1973b. Is polio a model for consumer research? Nature 241: 247-9.
1975a. Is poliomyelitis a genetically-determined disease? I. A genetic model. Medical Hypotheses 1: 23-32.
1975b. Is poliomyelitis a genetically-determined disease? II. A critical examination of the epidemiological data. Medical Hypotheses 1: 35—42.
1975c. Risk of live poliovirus in immunodeficient children. Journal OfPediatrics 87: 52-3.
1976a. Is poliomyelitis an auto-allergic disease triggered by virus? Medical Hypotheses 2: 262-8.
1976b. Provocation poliomyelitis and entry of poliovirus to the CNS. Medical Hypotheses 2: 269-74.
1978a. Abortive poliomyelitis or minor illness as a clue to genetic susceptibility. Medical Microbiology and Immunology 166: 37—42.
1978b. Polio immunization: Benefits and risks. Journal of Family Practice 7: 469—74.
1979. Poliomyelitis in the fetus and the newborn. A comment on the new understanding of the pathogenesis. Clinical Pediatrics 18: 33—8.
1981. Provocation poliomyelitis: Neglected clinical observations from 1914 to 1950. Bulletin of the History of Medicine 55: 543—57.
1984. The popularity of injections in the Third World: Origins and consequences. Social Science and Medicine 19: 911—15.
1985. Provocation of poliomyelitis by multiple injections. Transactions of the Royal Society for Tropical Medicine and Hygiene 79: 355-8.
1989. Poliomyelitis in developing countries: Lower limb paralysis and injections. Transactions of the Royal Society for Tropical Medicine and Hygiene 83: 545—9.
1990. Incubation of poliomyelitis as calculated from the time of entry into the central nervous system via the peripheral nerve pathways. Reviews of Infectious Diseases 12: 547—56.