117 Rheumatic Fever and Rheumatic Heart Disease
Acute rheumatic fever is a noncontagious disease characterized by febrile, nonsuppurative inflammation, primarily of articular and cardiac tissues, less frequently affecting the skin and brain.
The cerebral manifestation - Sydenham’s chorea - and the superficial manifestations — subcutaneous nodules and erythema marginatum - are limited to children and young adults.Etiology and Treatment
The disease is caused by infection, most often of the throat, with type A beta-hemolytic strains of streptococcus. Fever, migratory joint pains and tachycardia, the most frequent symptoms, typically begin 1 to 3 weeks after the onset Ofuntreated streptococcal pharyngitis. However, only 0.1 to 3.0 percent of untreated bouts of this infection result in a first attack of rheumatic fever. Consequently, various largely unidentified permissive factors must participate in initiating the immunologic pathogenesis of the disease.
First attacks of acute rheumatic fever can be prevented by timely treatment of the streptococcal infection with penicillin or another appropriate antibiotic, but such treatment does not influence the course of the disease once it has begun. Rheumatic fever recurs only as a result of a new infection with a pathogenic strain of streptococcus. Prophylactic antibiotic treatment diminishes, but does not eradicate recurrences (Taranta et al. 1964). The shorter the interval since the previous bout of rheumatic fever, the greater is the likelihood that a new attack will be elicited. An infection that occurs within 2 years of an attack has a 20 to 25 percent chance of inducing a recurrence. If the first attack does not affect the heart, a recurrence usually spares it as well, but if the heart has been involved, a second bout it likely to result in greater damage (Spagnuolo, Pasternack, and Taranta 1971). An attack of rheumatic fever usually lasts several weeks, but is rarely fatal.
Death most often is a consequence of chronic heart failure, which is the end result of damage to heart valves (predominantly the mitral and aortic valve). Rheumatic heart disease in about one-half the cases develops in the absence of any history of acute rheumatic fever, the infection having slightly initiated the pathogenic immunologic mechanism in the heart (Vendsborg, Hansen, and Olesen 1968).History
Clinical Manifestations and Diagnosis
The major clinical manifestations of rheumatic fever were first described separately, their relationships not being recognized until the ninteenth century. Thomas Sydenham in 1685 distinguished an acute, febrile polyarthritis “chiefly attacking the young and vigorous” from gout. One year later, he described as “St. Vitus’ dance” the neurological disorder that is now called Sydenham’s chorea (Murphy 1943). It was Richard Bright who in 1839 first connected the condition with rheumatic fever (Schechter 1935).
In 1797, Matthew Baillie of London noted a thickening of some heart valves in autopsies of patients who had had acute rheumatism, and a few years later David Dundas, surgeon to King George III, described nine cases of “a peculiar disease of the heart” that “is always the consequence of, or is connected with, rheumatic affection” (Dundas 1809). Four years later, William C. Wells, also of London, published a series of 16 cases of “rheumatism of the heart” (median age, 15 years), and added the description of subcutaneous nodules. However, the occurrence of nodules was largely ignored until a comprehensive study by Thomas Barlow and Francis Wamer was published in 1881 (Benedek 1984).
Before the introduction of auscultation by Ren6 T. Laennec in 1818, rheumatic heart disease was recognized from abnormalities of the pulse, respiration, and palpation of the chest in the presence or recent history of fever and joint pains. Laennec had described murmurs caused by deformities of the mitral valves. In 1835 James Hope also described murmurs that originated from the other valves and concluded that rheumatic fever is the most frequent cause (Hope 1846).
This opinion was soon confirmed by Jean B. Bouillaud. The “Aschoff nodule,” the myocardial granuloma that came to be considered pathognomonic of rheumatic carditis, had been recognized as early as 1883, but was described definitively by Ludwig Aschoff of Marburg only in 1904 (Benedek 1984).Bacteriologic studies, beginning in the 1870s, were made on blood and joint fluid aspirates. This approach Wasjustified in 1883 by the demonstration of the cause of gonococcal arthritis. The normal bacterial flora of the throat was not understood. Yet contrary to most investigators of the time, a Berlin physician writing at the turn of the twentieth century concluded that because one finds the same bacteria in the throats of persons with or without rheumatic fever, the disease must be caused not by a specific microbe but by a peculiar reactivity of susceptible individuals.
When Homer F. Swift of New York began his investigations of the cause of rheumatic fever in 1916, he was still culturing blood and joint fluid. In retrospect, the successful cultures that prolonged efforts to find a directly infectious agent (rather than an immunologic incitor) were due either to contamination or to the presence of bacterial endocarditis, an infection that usually is superimposed on rheumatic or Congential heart disease. By 1928 Swift had concluded that an allergic response to repeated streptococcal infections is the most likely cause of rheumatic fever, but erroneously believed that nonhemolytic strains were the principal pathogens. The investigations begun by Alvin F. Cobum in New York in the mid-1920s resulted in the correction and extension of Swift’s conclusions. On the basis of detailed epidemiological correlations of the bacterial flora of the throat with the onset of initial and recurrent bouts of rheumatic fever, Coburn inferred that the true pathogen is the hemolytic streptococcus, serologic type A (Benedek 1987). The hypothesis that the disease is mediated immunologically was supported by the discovery by E.
W. Todd in London of antibodies to streptococci in the blood of rheumatic fever patients (Todd 1932).Early Epidemiological Studies
The first statistical report, by John Haygarth in 1805, found that 4.5 percent of the admissions to the Chester Infirmary between 1767 and 1801 had “rheumatism” and that 36 percent of those, or 1.6 percent of the total, had acute febrile rheumatism or “rheu- matick fever.” How many of these actually were cases of this disease is uncertain (a problem that continued to vex many surveys). Eleven of the 70 cases of whom age was recorded involved patients 50 to 70 years old, and unequivocal symptoms of heart failure were not described even in fatalities.
Most reports since then have also described the experience in an individual hospital. Regional surveys and mandatory reporting of rheumatic fever have been rare, occurring mainly in Great Britain, Scandinavia, and the United States. Nearly a century after Haygarth’s monograph, a report on the occurrence of “rheumatism” at St. Bartholomew’s Hospital, London, demonstrated the vagaries of diagnosis in more detail, as well as the great prevalence of rheumatic fever. During the 15-year span 1863 to 1877, an average of 323 patients with “rheumatism” were admitted annually. This constituted about 14 percent of all medical admissions. Beginning in 1867, gonorrheal rheumatism and rhematoid arthritis were diagnosed separately. However, this change only slightly reduced the cases of presumed acute rheumatic fever with or without heart disease - to 311 per year. The associated mortality was 1.3 percent (Southey 1878). This result is consistent with more recent U.S. data according to which the acute mortality has ranged from 3.5 percent during 193542 to 0.9 percent during 1951-8 (Mayer et al. 1963). At St. Bartholomew’s during 1867-77, a total of only 716 cases of scarlet fever (also caused by infection with the hemolytic streptococcus) were admitted, and the mortality among these was 14.0 percent (Southey 1878).
Acute rheumatic fever occurred more frequently in older persons in the nineteenth century than in the more recent preantibiotic period. A questionnaire sent to physicians by the British Medical Association during 1882-6 regarding their cases of rheumatic fever indicated the mean age of an attack among 647 cases to have been 25.4 years, with 4 percent of the patients over 60 years of age (Whipham 1888). Of 400 cases admitted to Roosevelt Hospital in New York during 1872-82, 7 percent of the attacks occurred in patients older than 55. By contrast, 25 percent of first attacks occurred between ages 20 and 25, whereas 49 percent of first attacks and 34 percent of all attacks occurred in the third decade of life (May 1884). The latter is similar to the experience at Bellevue Hospital in New York 40 years later, where, as Table VIIL 117.1 shows, 34.5 percent of the cases of acute rheumatic fever were in the third decade. By the 1930s, however, only 13.8 percent of patients admitted to Philadelphia hospitals for acute rheumatic fever were in their third decade. Similarly, a review of 3,129 cases in New York, the majority of whom had their first attack between 1920 and 1940, showed a mean age of onset of 15 years (Lambert 1920).
In the 1880s, it was estimated in London that about 20 percent of patients without symptoms or history of rheumatic fever who were admitted to a hospital for any reason had a sibling or parent who had had rheumatic fever; such familial cases were present in about 35 percent of the patients who were hospitalized because of rheumatic fever (Garrod and Table VIII.117.1. Age distribution of admissions for acute rheumatic fever
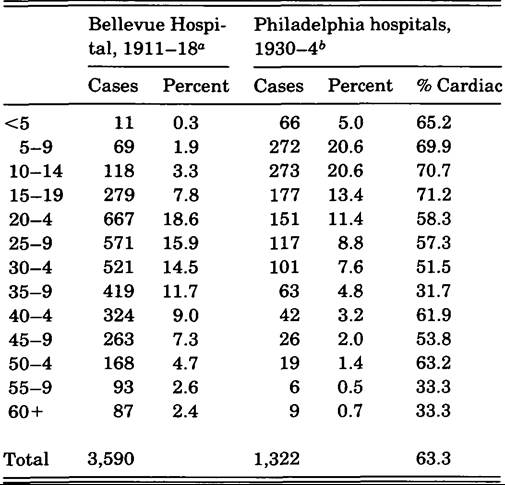
Sources: Data from “Lambert (1920); and 6Hedley (1940).
Cooke 1888). It had been noted in a British Medical Association survey that rheumatic fever “greatly preponderates in the lower over the middle and upper classes” (Whipham 1888).
The occurrence of multiple cases in a family was at first attributed to inheritance. As bacteriologic findings came to be accepted in the 1880s and 1890s, however, the concept that both familial occurrence and the association with poverty could best be explained by the easier spread of an infectious agent in crowded living conditions also became accepted. The possibility of racial predisposition was considered because of the greater prevalence of rheumatic fever in populations as disparate as American blacks, South African Bantus, and New Zealand Maoris as compared to white nationals. Most investigators, however, concluded that susceptibility was due to the greater poverty and poorer housing of certain racial groups in various societies, although several investigations have suggested that there is a heritable factor that influences susceptibility to rheumatic fever (Wilson and Schweitzer 1954).The importance of crowded living conditions gained further attention because of the prevalence of the diagnosis of rheumatic fever in military encampments during the First World War. Between April 1917 and December 1919, for example, 24,770 U.S. soldiers, representing 27 percent of all rheumato- Iogic cases, received this diagnosis. Crowded training camps were believed to have contributed to the disproportionately large percentage of cases (Hench and Boland 1946). The development of epidemiological data about rheumatic fever has been difficult because the acute phase of the disease may be brief or actually imperceptible, so that its occurrence may become recognized only from findings of valvular heart disease, perhaps years later in an uncertain proportion of the cases. Many estimates of the prevalence of rheumatic fever have been extrapolated from the prevalence of heart disease in those between the ages of 5 and 19 years, because their disease is most likely to be rheumatic. Widely differing diagnostic criteria, examining techniques, and reporting practices have made epidemiological comparisons unreliable. This problem began to be addressed in 1943 by the Cardiovascular Diseases Subcommittee of the [U.S.] National Research Council, which sought more precise diagnostic criteria so as to assess the problem of rheumatic fever in military training camps. In response, T Duckett Jones, a Boston cardiologist, devised a set of five “major” and seven “minor” criteria and proposed that “any single major manifestation with at least two of the minor manifestations would seem to place the diagnosis on reasonably safe grounds.” The Jones criteria received international acceptance quite rapidly and have been modified twice. The main revision in 1955 altered the importance that was assigned to some clinical signs, whereas the revision in 1965 placed increased importance on laboratory evidence of recent streptococcal infection (Stollerman et al. 1965).
Treatment
Salicylate preparations introduced between 1876 and 1879 were found to be particularly effective in counteracting the fever and joint pain of acute rheumatic fever. In 1899 aspirin came on the market, and for the next 50 years the basic treatment consisted of the maximum tolerated dose of either sodium salicylate or aspirin (Rodnan and Benedek 1970). Greater understanding of the cause of rheumatic fever did not have an immediate effect on its treatment because there was no way to eradicate a streptococcal infection. Sulfanilamide was found to prevent recurrences when taken prophylactically (Swift, Moen, and Hirst 1938; Thomas and France 1939). Penicillin became available in 1945 and quickly proved to be safer and more reliable as a preventive agent (Spink et al. 1946). The most reliable prophylactic method, a monthly injection of slowly excreted benzathine penicillin, was introduced in 1951.
The introduction in 1949 of cortisone and corticotropin was perceived as the first possible improvement over salicylate therapy for acute rheumatic fever. During the first few years in which these hormones were available, most investigators found that control of fever and joint pain was achieved more rapidly with these drugs than with salicylates; moreover, if given early enough, they seemed to minimize heart damage. Uncertainty about the latter impression, however, led to the establishment in 1955 of an elaborate Anglo-American prospective therapeutic comparison of salicylate with cortisone or corticotropin therapy. After 10 years, it was concluded that the long-term results from both modalities were similar (U.K. and U.S. Joint Report 1965).
Decline of Rheumatic Fever
London physician G. B. Longstaff (1905) may have been the first to suggest that the prevalence of rheumatic fever was decreasing. He deduced this from death certificates in England and Wales during 1881-1900. During these 20 years, 51,666 deaths were attributed to “rheumatic fever” or “rheumatism of the heart,” and 3.3 times as many (171,298) to “valvular disease of the heart.” In comparing the 5-year periods 1881-5 and 1896-1900, death rates per million due to rheumatic fever declined 15.6 percent, from 97.6 to 82.4, and those for “residual rheumatism” declined 19.1 percent from 35.0 to 28.3. Data collected by J. A. Glover (1930) for the same region showed a lower incidence of deaths for 1901 than Longstaffhad calculated (67 per million), but indicated continuity of the decline: to 46 per million in 1910 and 38 per million in 1928.
The two most common sources of epidemiological data other than death reports have been hospital admissions and recurrence rates among patients who were being followed in rheumatic fever clinics. In order for hospitalization data to be intrinsically comparable, one must assume a socioeconomically stable service area and consistent admissions policies, both of which assumptions are risky. Clinic data tend to yield the most detailed information, but if the clinic is effective, its prevalence information cannot be extrapolated to communities that lack similar services.
Annual admissions data for rheumatic fever were recorded between 1906 and 1925 for hospitals in Montreal, Boston, New York, New Orleans, and the Panama Canal Zone. A comparison of the proportion of total admissions for rheumatic fever between 1906-8 and 1923-5, as reflected in Table VIΠ.117.2, shows a decline from 59 percent (New York Bellevue) to 79 percent (New Orleans Charity) (Seegal and Seegal 1927).
Table VIΠ.117.2. Cases Ofrheumatic fever per 1,000 admissions, various hospitals
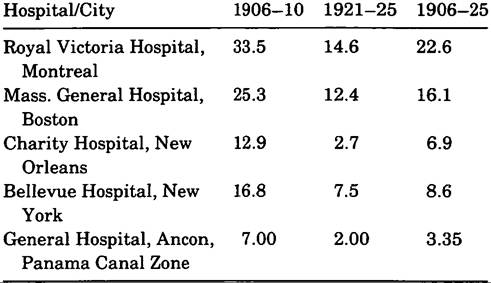
Source: Data from Seegal and Seegal (1927).
A comparison of the prevalence of rheumatic fever among U.S. military personnel during the two world wars shows that, as serious as the problem was during World War II, this diagnosis was made in only 10 percent as many army and 38 percent as many navy personnel. The contribution of more precise diagnosis and prophylactic programs to this improvement is uncertain.
The lengthiest clinical evaluation of rheumatic fever patients was carried out by M. G. Wilson and collaborators (1958) in New York. Beginning in 1916 and continuing in the same area for 40 years, it reported a steady decline in recurrences of rheumatic fever, unrelated to treatment. During 1921— 43, 25 percent of children 6.to 13 years of age and 6.1 percent of those aged 14 to 20 suffered recurrences, whereas during 1944-56 only 15.1 percent of the younger and 2.8 percent of the older age group were so affected.
Antimicrobial prophylaxis began to be used in 1952. Yet the age-adjusted recurrence rate for the 5 years 1942-6 was 7.9 percent, and for 1952-6 it was 6.1 percent; this difference was not significant. The socioeconomic circumstances of the area served by the clinic had improved during these decades, but no improvement in the recurrence rate was observed in the poorest segment of the population (Wilson, Lim, and Birch 1958).
A study of the economic correlates of the occurrence of primary and recurrent rheumatic fever in Baltimore during 1960-4 also demonstrated a strong correlation between low economic status and the occurrence of the disease, but only among the white subjects. The annual incidence was consistently greater among blacks, with only slight improvement related to higher socioeconomic category, whereas the incidence among whites diminished markedly with higher socioeconomic category. Thus, the annual incidence of rheumatic fever among blacks in the lowest fifth on the socioeconomic scale was 56 percent greater than among comparable whites, whereas the difference reached 478 percent when the most affluent fifths were compared (Gordis, Lilien- feld, and Rodriguez 1969).
In weighing the relative importance of rheumatic fever and rheumatic heart disease against other potentially lethal problems of childhood, we find that in the United States during 1939-41, the pair still ranked second, behind accidents, as the leading causes of death in the 10- to 14-year age group. There was a significant sex- and race-related gradient, from 11.2 deaths per 100,000 white boys to 17.4 deaths per 100,000 nonwhite girls (Wolff 1951). This amounted to an average of 4,000 deaths per year for that period. But by 1972-4, an average of only 179 deaths were reported annually, and by 1982-4, deaths had declined to 78 cases per year. Similarly, as Table VIII.117.3 indicates, the reported national incidence of rheumatic fever declined from 10,470 cases in 1961 to 2,793 cases in 1971 and 264 cases in 1981.
Geography
Rheumatic fever was thought to be rare in the tropics, as judged by observations on English troops and native populations in India in the mid-nineteenth century. Seeming to confirm that view were clinical and autopsy reports, primarily from India and the Malay Peninsula, which started to appear in the 1890s and were still cited in the 1930s (Clarke 1930). But these publications are somewhat perplexing, for beginning in 1925, substantial numbers of cases of rheumatic heart disease were being reported from tropical India.
Nevertheless, rheumatic fever has been found to occur less frequently in tropical than in temperate regions despite the fact that poverty, aspects of which appear to facilitate the occurrence of the disease, is in general more prevalent in the tropics. Thus, observations on military personnel that minimize the economic factor have shown a lower incidence in tropical encampments. For example, the mean incidence of rheumatic fever among white U.S. Army enlisted men stationed in the United States during 1913-25 was 5.00 plus or minus 2.46 per 1,000, whereas the incidence among similar personnel stationed in the Philippines was 1.74 plus or minus 1.23 per 1,000 (Faulkner and White 1924). Paradoxically, however, during the decade 1914-23 there were slightly more admissions for rheumatic fever to the General Hospital of Manila than to the Johns Hopkins Hospital in Baltimore - 7.90 versus 7.19 per 1,000 medical admissions (Seegal and Seegal 1927).
A north-to-south declining gradient of rheumatic fever within the United States was suggested during the 1920s (Harrison and Levine 1924). This was confirmed by numerous studies, including one in which the prevalence of rheumatic heart disease was compared among Indian children on reservations in Montana, Wyoming, and Arizona (Paul and Dixon 1937). A similar gradient has been reported from China. An altitude gradient has been demonstrated in Kenya for hospitalizations for acute rheumatic fever, and in Mexico for the proportion of rheumatic heart disease among cardiac patients. In both countries there was significantly more disease in the more temperate highlands.
The “classical” manifestations of rheumatic fever were described in northern Europe, and whether its acute manifestations differ in the tropics has long been debated. If one considers, however, the wide variation in the frequency with which various acute manifestations of the disease have occurred in temperate regions, as presented in Table VIII.117.3, it seems doubtful that there are consistent biological differences in the presentation of rheumatic fever in the tropics. Some of the reported inconsistencies reflect selection biases related to cultural attitudes and medical and other resources, whereas others reflect over- or underdiagnosis. For example, the fact that virtually all of the patients in a small series of cases from Nigeria and Uganda had carditis probably indicates that childhood cases of lesser severity were simply not seen rather than nonexistent.
The wide range of the occurrence of “arthritis” in rheumatic fever cases may be attributed in part to the differentiation by some authors between objective signs of joint inflammation and mere arthralgia. Nevertheless, there can be striking differences in the occurrence of arthritis, even when rigorous diagnostic criteria may be assumed; for example, 42 percent and 71 percent of the patients had arthritis in two series of cases at two different times from Toronto. But the extreme variations in the occurrence of chorea - ranging from 2 percent to 52 percent - are the most inexplicable. Erythema marginatum is rarely described in dark-skinned children, but this eruption is sufficiently uncommon in fair-skinned individuals that, assuming some underdiagnosis in the former, a significant difference seems unlikely.
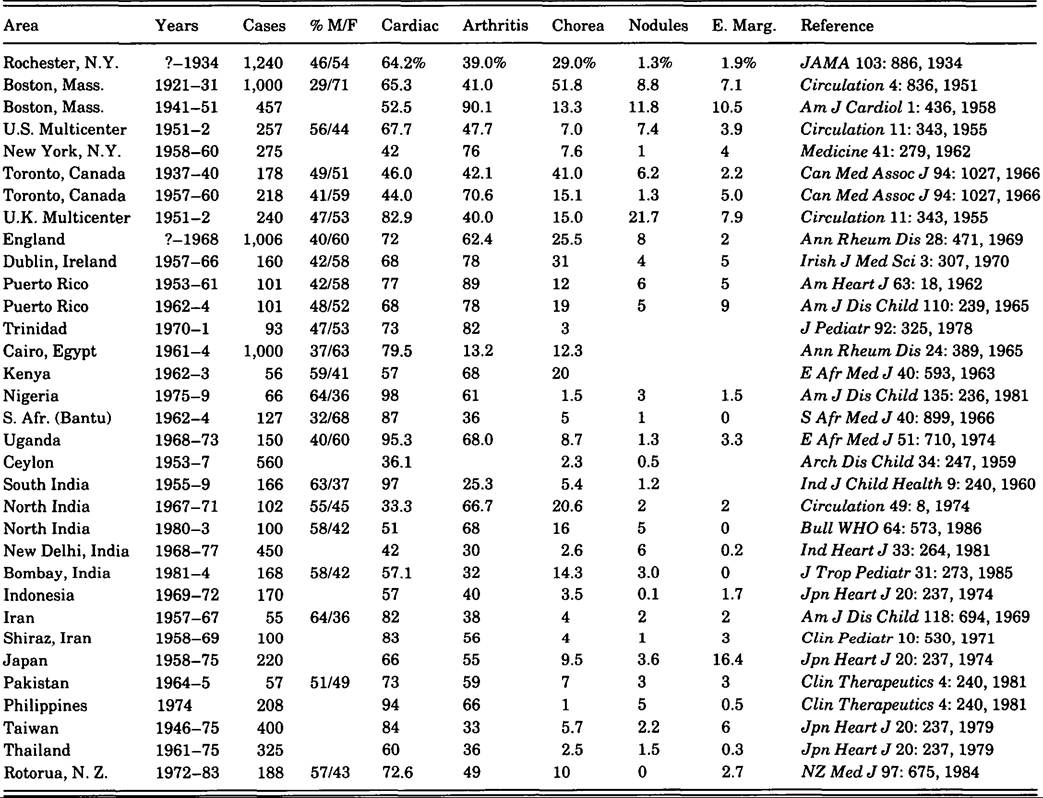
The relationship of subcutaneous nodules to carditis may indicate real geographic differences in disease expression. Nodules have occurred in 8 to 12 percent of several large series of cases from temperate regions (Benedek 1984), whereas they have been less common in others and have consistently been rare in the tropics. In temperate climates nodules are almost always associated with acute carditis and may be predictive of more severe valve damage. Thus, according to the long-term experience of Wilson and W. Lim (1957) in New York, 3 percent of cases of mitral insufficiency, 9 percent of cases of combined mitral insufficiency and stenosis, and 30 percent of cases of combined mitral and aortic valve damage had exhibited nodules during the acute phase of illness. In tropical areas there is a weaker association between the occurrence of nodules and carditis and a difference in the valvular involvement, or at least this seems to be the case of India. There, carditis not only results in permanent valve injury more rapidly and is more likely to be acutely fatal, but also has a peculiar tendency to cause pure mitral stenosis. This has been described repeatedly since 1935. According to the largest reported experience involving 2,050 cases of rheumatic heart disease in New Delhi, 81 percent of whom were below 30 years of age, 43.5 percent had pure mitral stenosis (Wilson et al. 1958). Reports from other countries do not resolve the question of whether this finding represents an ethnic difference or is a result of delayed initial medical care.
Rheumatic Heart Disease and Its Surgical Repair
Wilson and associates evaluated 385 patients up to 49 years of age who had heart murmurs and had had rheumatic fever before the age of 20. Fully 89 percent were asymptomatic; 45 percent of the cohort had pure mitral insufficiency; 41.8 percent had combined mitral insufficiency and stenosis; 10.3 percent had both mitral lesions and aortic insufficiency; and 2.9 percent had double mitral and double aortic valve defects (Gordis et al. 1969). Of 78 fatal cases from the population of which those just mentioned were among the survivors, 15.4 percent had only mitral insufficiency, 37.2 percent had mitral insufficiency and stenosis, and 47.3 percent also had aortic insufficiency (Magida and Streitfeld 1957).
The surgical treatment of Theumatically damaged heart valves began in the late 1940s when Dwight E. Harken in Boston performed the first successful mitral commissurotomy (Harken et al. 1948). The procedure was improved by Charles P. Bailey of Philadelphia a year later (Bailey et al. 1960). This was “closed” heart surgery. No attempt to repair a damaged aortic valve was possible until an oxygenating system to bypass blood temporarily around the heart was developed; this technique made “open” heart surgery possible. The first practical apparatus was employed by John W. Kirklin. The first valve operations to ameliorate aortic insufficiency were performed by Bailey in 1959 and to correct aortic stenosis in the same year by Donald G. Mulder in Los Angeles. The next technical phase was the replacement of an active valve. This began with the ball valve devised by Albert Starr and Lowell Edwards (1961). Such plastic valves, however, tend to destroy red blood cells, and thus valves were developed with leaflets of pig, cattle, or sheep tissue. This type of prosthesis was first inserted to replace an aortic valve in 1965, and a mitral valve in 1967, both by A. Carpentier in Paris.
In 1983 about 16,000 mitral and 33,000 aortic valve replacements were performed in the United States. However, the cause of the injury, particularly of the aortic valve, has gradually shifted from rheumatic to other varieties of heart disease (Gillum 1986).
Thomas G. Benedek
Bibliography
Arora, R., et al. 1981. Clinical profile of rheumatic fever and rheumatic heart disease: A study of 2,500 cases. Indian Heart Journal 33: 264—9.
Bailey, C. P., J. Zimmerman, and W. Likoff. 1960. The complete relief of mitral stenosis: Ten years of progress toward this goal. Diseases of the Chest 37: 543-60.
Benedek, T. G. 1984. Subcutaneous nodules and the differentiation of rheumatoid arthritis from rheumatic fever. Seminars in Arthritis and Rheumatism 13: 306-21.
1987. A century of American rheumatology. Annals of Internal Medicine 106: 307—12.
Clarke, J. T. 1930. The geographical distribution of rheumatic fever. Journal of Tropical Medicine and Hygiene 33: 249-57.
Dimdas, D. 1809. An account of a peculiar disease of the heart. Medico-Chirurgical Transactions 1: 36—46.
Faulkner, J. M., annd P. D. White. 1924. The incidence of rheumatic fever, chorea and rheumatic heart disease. Journal of the American Medical Association 83: 425-6.
Garrod, A. E., and E. H. Cooke. 1888. Frequency of rheumatic family histories amongst non-rheumatic patients. Lancet 2: 110.
Gillum, R. F. 1986. Trends in acute rheumatic fever and chronic rheumatic heart disease: A national perspective. American Heart Journal 111: 430—2.
Glover, J. A. 1930. I. The incidence of acute rheumatism. Milroy lectures on the incidence of rheumatic fever, 1: 499-505.
Gordis1 L., A. Lilienfeld1 and R. Rodriguez. 1969. Studies in the epidemiology and preventability of rheumatic fever. Journal of Chronic Diseases 21: 645—66.
Harken, D. E., et al. 1948. The surgical treatment of mitral stenosis. I. Valvuloplasty. New England Journal OfMedicine 239: 801—9.
Harris, T. R., and S. A. Levine. 1924. Notes on the regional distribution of rheumatic fever and rheumatic heart disease in the United States. Southern Medical Journal 12: 914-15.
Hedley, O. F. 1940. Rheumatic heart disease in Philadelphia hospitals, part II. Public Health Reports 55: 1647-91.
Hench, P. S., and E. W. Boland. 1946. The management of chronic arthritis and other rheumatic disorders among soldiers of the United States Army. Annals of Internal Medicine 24: 808-25.
Hope, J. 1846. A treatise on the diseases of the heart and great vessels, and on the affections which may be mistaken for them, 2d American edition, from 3d London edition, 95-113. Philadelphia.
Lambert, A. 1920. The incidence of acute rheumatic fever at Bellevue Hospital. Journal OftheAmerican Medical Association 74: 993-5.
Longstaff1 G. B. 1905. A contribution to the etiology of rheumatic fever. Transactions of the Epidemiological Society of London, new ser., 24: 33-83.
Magida, M. G., and F. H. Streitfeld. 1957. The natural history of rheumatic heart disease in the third, fourth and fifth decades of life. II. Prognosis with special reference to morbidity. Circulation 16: 713-22.
May, C. H. 1884. Statistics of four hundred cases of rheumatism, with special reference to treatment: treated at the Roosevelt Hospital. Medical Record 25: 57-62, 87-93, 116-21, 173-8.
Mayer, F. E., et al. 1963. Declining severity of first attack of rheumatic fever. American Journal of the Diseases of Childhood 105: 146-52.
Murphy, G. E. 1943. The evolution of our knowledge of rheumatic fever. Bulletin of the History of Medicine 14: 123-47.
Paul, J. R., and G. L. Dixon. 1937. Climate and rheumatic heart disease: A survey among American Indian school children in northern and southern localities. Journal of the American Medical Association 108: 2096-100.
Rodnan, G. P., and T. G. Benedek. 1970. The early history of antirheumatic drugs. Arthritis and Rheumatism 13: 145-65.
Schechter, D. C. 1975. St. Vitus’ dance and rheumatic disease. New York State Journal of Medicine 75: 1091-102.
Seegal, D., and B. C. Seegal. 1927. Studies in the epidemiology of rheumatic fever. Journal of the American Medical Association 89: 11-17.
Southey, R. 1878. Observations on acute rheumatism. St. Bartholomew’s Hospital Reports 14: 1—22.
Spagnuolo, M., B. Pastemack, and A. Taranta. 1971. Risk of rheumatic fever recurrences after streptococcal infections. NewEngland Journal OfMedicine 285:641-7.
Spink, W. W., et al. 1946. Sulfadiazine and penicillin for hemolytic streptococcus infections of the upper respiratory tract. Archives OfInternal Medicine 77: 260—94.
Starr, A., and M. L. Edwards. 1961. Mitral replacement: Clinical experience with a ball-valve prosthesis. Annals OfSurgery 154: 726-40.
Stollerman, G. H., et al. 1965. Jones criteria (revised) for guidance in the diagnosis of rheumatic fever. Circulation 32: 664—8.
Swift, H. F., J. K. Moen, and G. K. Hirst. 1938. The action of sulfanilamide in rheumatic fever. Journal of the American Medical Association 110: 426—34.
Taranta, A., et al. 1964. Rheumatic fever in children and adolescents. IV. Relationship of the rheumatic fever recurrence rate per streptococcal infection to the titers of streptococcal antibodies. Annals of Internal Medicine 60 (Supplement 5): 47-57.
Thomas, C. B., and R. France. 1939. A preliminary report of the prophylactic use of sulfanilamide in patients susceptible to rheumatic fever. Bulletin of the Johns Hopkins Hospital 64: 67-77.
Todd, E. W., 1932. Antigenic streptococcal haemolysin. Journal OfExperimental Medicine 55: 267—80.
U.K. and U.S. Joint Report. 1965. The natural history of rheumatic fever and rheumatic heart disease: Cooperative clinical trial of ACTH, cortisone, and aspirin. Circulation 32: 457-76.
Vendsborg, P., L. F. Hansen, and K. H. Olesen. 1968. Decreasing incidence of a history of acute rheumatic fever in chronic heart disease. Cardiologia 53: 332—40.
Whipham, T. 1888. Reports of the Collective Investigation Committee of the British Medical Association. III. Acute rheumatism. British Medical Journal i: 387-404.
Wilson, M. G., and M. Schweitzer. 1954. Pattern of hereditary susceptibility in rheumatic fever. Circulation 10: 699-704.
Wilson, M. G., and W N. Lim. 1957. The natural history of rheumatic heart disease in the third, fourth and fifth decades of life. I. Prognosis with special reference to survivorship. Circulation 16: 700—12.
Wilson, M. G., W N. Lim, and A. M. Birch. 1958. The decline of rheumatic fever: Recurrence rates of rheumatic fever among 782 children for twenty-one consecutive calendar years (1936-1956). Journal of Chronic Diseases 7: 183-97.
Wolff, G. 1951. Death toll from rheumatic fever in childhood. Journal of the American Medical Association 145: 719-24.