120 Rocky Mountain Spotted Fever and the Spotted Fever Group Diseases
Rocky Mountain spotted fever is a severe, acute, rickettsial disease transmitted by ticks and limited to the Western Hemisphere. Its major symptoms are similar to those of epidemic typhus, but its rash covers the entire body, including the face, the palms of the hands, and the soles of the feet.
Between 20 and 25 percent of untreated victims die, making Rocky Mountain spotted fever the most severe rickettsial infection in the Americas. First identified in the Rocky Mountain region of the United States, this place name has never been dislodged, even though it is inaccurate and even misleading.Etiology and Epidemiology
The severity with which Rocky Mountain spotted fever treats its victims underscores its natural existence as an infection of ticks and their mammalian hosts. The microbial cause of the disease, Rickettsia rickettsii, normally inhabits ixodid, or hard shell, ticks, apparently causing little harm to the host. Although small mammals are susceptible to a mild infection with R. rickettsii and may transmit it to uninfected ticks, the principal means by which the organism is maintained in nature is from one generation to the next in the eggs of the female tick.
The epidemiology of Rocky Mountain spotted fever is linked to areas favorable for the habitation of the vector ticks. The Rocky Mountain wood tick, Derma- centor andersoni, and the American dog tick, Derma- centor variabilis, are the most common vectors in the United States, although the Lone Star tick, Ambly- omτna americanum, also transmits the disease in the south central and southeastern parts of the United States. Two other ticks, Rhipicephalus sanguineus and Amblyomma Cajennense, also carry the disease in Mexico, Central America, and South America. Only a small percentage of ticks - generally less than 5 percent - are usually infective.
Humans typically contract Rocky Mountain spotted fever when they accidentally become a part of the disease’s biosystem.
In the western United States, hikers, backpackers, and the like may become subjected to infection when traveling in areas where ticks are plentiful, especially during the spring months. In the eastern United States, where most cases now occur, changing land-use patterns have brought humans into the habitat of the tick. The development of suburban housing developments and the transformation of agricultural land into wooded recreation areas are two examples.Rocky Mountain spotted fever characteristically appears in “islands” of infection. During early research on a particularly virulent form in Montana’s Bitterroot Valley, for example, investigators were baffled by the fact that Rocky Mountain spotted fever appeared on the west side of the Bitterroot River but not on the east side (see Map VIII.120.1). Recently, Rocky Mountain Laboratory investigator Willy Burgdorfer has shown that this peculiar epidemiological occurrence is related to an antigenic “interference phenomenon.” Nonpathogenic rickett- siae in the ovaries of ticks on the east side of the river “interfere” with the establishment of pathogenic rickettsiae in these tissues, thus preventing the pathogenic R. rickettsii from being passed on to the next generation of ticks.
Distribution and Incidence
Known only in the Western Hemisphere, Rocky Mountain spotted fever has been identified in Canada, the United States, Mexico, Costa Rica, Panama, Brazil, and Colombia. Before 1940, most cases were reported in the Rocky Mountain region, but since that time, the number of cases in the southeastern and southwestern United States (sometimes called the “tick belt” region) has far outstripped those reported from the west. In the 1970s, case incidence in the United States began to rise, reaching a peak of 1,192 cases in 1981. In recent years, the number of cases has declined slightly and leveled off. At present, Oklahoma has the highest infection rate in relation to its population, whereas North Carolina reports the largest number of cases.
A small number of cases continues to occur in Canada. In Mexico and Central and South America, the disease is poorly reported, and consequently it is difficult to estimate its actual incidence in these areas.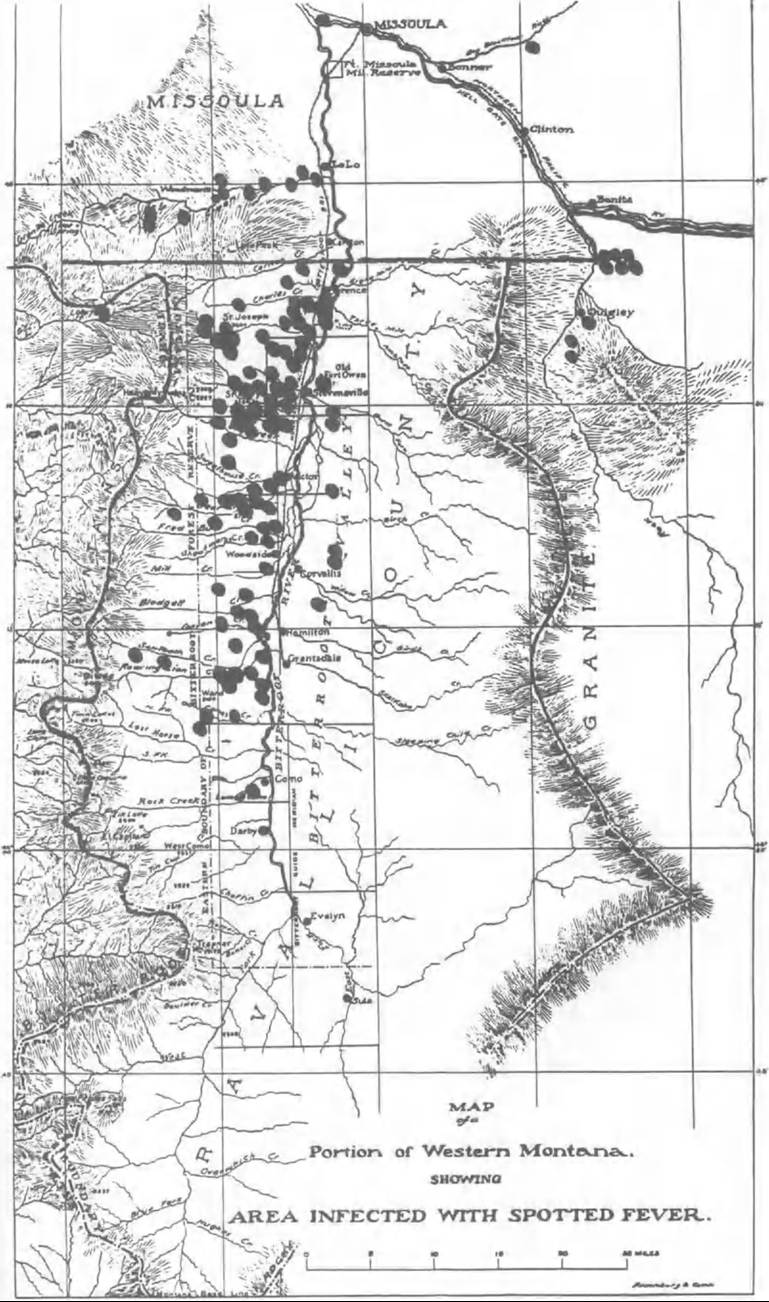
Map VIII.120.1. Epidemiological map of Rocky Mountain spotted fever in Bitterroot Valley, Montana, 1902. Recorded cases are highlighted to show the predominant distribution of cases on the west side of the valley. (From Wilson and Chowning 1904.)
Clinical Manifestations
After an incubation period of from 3 to 12 days, typical typhuslike symptoms appear abruptly, severe headache, joint and back pains, prostration, and a high fever. About the fourth day of fever, the characteristic skin rash appears. Usually beginning on the wrist and ankles, it spreads to cover the entire body. Because few diseases cause rashes on the palms of the hands and the soles of the feet, this sign, when accompanied by high fever and history of tick exposure, is considered diagnostic. The fever continues for 2 to 3 weeks, usually subsiding gradually in cases that recover. In fatal cases, neurological symptoms of deafness, confusion, delirium, and coma are accompanied by circulatory collapse, and, often, kidney failure. In addition, the rash may darken, becoming almost black, and may spread, becoming confluent in some cases. These characteristics contributed to two early names for the disease, “black measles” and “blue disease.”
If diagnosed early in the course of illness, Rocky Mountain spotted fever may be treated effectively with broad-spectrum antibiotics. Patients at risk of dying are usually those in whom the disease is not diagnosed in time to begin effective treatment. On their first visit to a physician, such patients do not report a history of tick exposure, do not yet have a visible rash, and often complain of abdominal symptoms that may be confused with other illnesses.
At special risk are people who suffer from glucose- 6-phosphate dehydrogenase (G6PD) deficiency, a genetic-linked disorder, which has a high frequency in black males relative to most other peoples and to black females. Thus mortality rates from Rocky Mountain spotted fever are significantly higher for black males than for the general population.History and Geography
Rocky Mountain spotted fever as a specific disease entity is essentially twentieth century in origin. Retrospective diagnoses have identified the disease in the eighteenth and nineteenth centuries, but the first reports differentiating it from other fevers were published only in the late 1890s. Pioneers traveling the western trails of North America encountered a disease in the spring variously known as “trail typhus,” “spotted fever,” “spotted typhus,” or other such descriptive names. Mortality varied from under 5 percent in Idaho to approximately 70 percent in the Bitterroot Valley of western Montana.
In 1901, public outcry for action against the deadly disease in the Bitterroot Valley stimulated the newly created Montana State Board of Health to Iatmch a scientific investigation of the disease. In 1902, two pathologists from the University of Minnesota suggested that the wood tick might be the vector of the disease, which they believed was caused by a protozoan organism. Their etiologic theory was discredited, but in 1906 the tick was independently confirmed as the disease vector by Howard Taylor Ricketts of the University of Chicago and by Walter King of the U.S. Public Health Service. Ricketts continued the investigations, seeking to produce a vaccine or therapeutic serum against the disease. In 1909, when funding for Ricketts’s research was delayed in the Montana state legislature, he accepted an invitation to study tabardillo, the Mexican typhus fever, in Mexico City. Tragically, he contracted typhus and died in May 1910.
Between 1910 and 1920, efforts to combat Rocky Mountain spotted fever focused on tick eradication programs.
Modeled on the successful tick control program that had eliminated Texas cattle fever throughout the South, the campaign failed against Rocky Mountain spotted fever for two reasons. The Texas cattle fever tick was a one-host tick, whereas the Rocky Mountain wood tick chose different hosts for each stage in its life cycle. This characteristic made control much more difficult. Second, cold spring weather in Montana interfered with livestock dipping when the ticks first emerged.In 1916 S. Burt Wolbach of Harvard University Medical School described the etiologic agent of Rocky Mountain spotted fever, which he labeled “a wholly new kind of micro-organism.” Wolbach originally named it Dermacentroxenus rickettsi, the genus name after its vector tick and the species name after Ricketts. Taxonomists later classified this organism in the same genus with the typhus germs, changing its name to Rickettsia rickettsii.
In 1921 the U.S. Public Health Service renewed the effort to prepare a vaccine against Rocky Mountain spotted fever. Workingjointly, physician Roscoe R. Spencer and entomologist Ralph R. Parker succeeded in 1924 in preparing a vaccine from infected ticks, the first successful vaccine made from the bodies of arthropod vectors. From 1925, when clinical trials began, through 1948, when effective antibiotics were introduced, the Spencer-Parker vaccine was the chief means of fighting Rocky Mountain spotted fever.
In 1931 the disease was discovered to exist on the eastern seaboard of the United States, and shortly thereafter, pockets of infection were identified in Sao Paulo, Brazil; in Tobia, Colombia; in Choix, Mexico; as well as in Canada and other areas of the Western Hemisphere. The original names by which the disease was known sometimes Imderscored its character as a “place” disease. For example, it was called febre maculosa brasileira but also “Sao Paulo typhus” in Brazil, “Tobia petechial fever” in Colombia, and fiebre de Choix as well as fiebre manchada in Mexico.
As additional information became known about other rickettsial diseases, numerous investigators suggested more appropriate names for the disease, such as tick-bome typhus, tick spotted typhus, American spotted fever, or, simply, spotted fever. None successfully supplanted Rocky Mountain spotted fever.After the introduction of the broad-spectrum antibiotics in 1948, Rocky Mountain spotted fever incidence in the United States dropped to about 250 cases per year, with only about 24 deaths. To some extent, the early and widespread use of antibiotics may have obscured the true incidence of the disease. Beginning in 1969 and continuing through the 1970s, the incidence of Rocky Mountain spotted fever rose inexorably in the United States, probably as a result of the development of suburban housing and the transformation of agricultural land into wooded recreational areas. Although this phenomenon was not reported from other countries of the hemisphere, it was reported in the Mediterranean basin, where boutonneuse fever, a related but milder spotted fever group disease, was known. The increase in Rocky Mountain spotted fever cases and deaths during the 1970s stimulated new research into diagnosis and prevention of the disease.
Unlike epidemic typhus, Rocky Mountain spotted fever poses no threat of erupting into epidemics. As a disease of nature, however, it is unlikely to be eradicated as a human hazard. If the public and physicians are alert to the possibility of infection during “tick seasons,” effective antibiotic therapy can be administered and Rocky Mountain spotted fever need not cause unnecessary loss of life.
Other Diseases of the Spotted Fever Group Three other major tick-bome rickettsioses are known throughout the world. Usually mild diseases, these three spotted fever group maladies are generally fatal only to the aged or debilitated patients. All exhibit a distinctive diagnostic characteristic, an eschar, or dark scab, that forms over the wound caused by the initial tick bite. Lymph nodes draining the eschar also swell and become tender.
Boutonneuse fever, named for the buttonlike eschar, was the earliest of these spotted fever group diseases identified. Described by Alfred Conor in North Africa in 1910, the disease has also been known by many other local names, including Mediterranean spotted fever, fieυre boutonneuse, Marseilles exanthematic fever, Indian tick-typhus, South African tick-bite fever, and Italian eruptive fever. Its most common etiologic agent is Rickettsia conorii, the species name given in honor of Conor. In recent decades, other variant spotted fever group strains have also been identified as causing this disease. A number of different ticks are responsible for its transmission, the most common being R. sanguineus. In Africa, many people apparently gain immunity during childhood through a mild infection, for the disease is primarily seen in tourists or in new residents. From its local names, it is apparent that boutonneuse fever is known from Africa throughout the Mediterranean basin and into India. During the 1970s an increase paralleling that of Rocky Mountain spotted fever in the United States was reported in the Mediterranean basin.
Siberian tick-typhus was first documented during the 1930s, when exploitation of Siberian forest and steppes brought many people into the habitat of its vector ticks. Transmitted by several species of ixodid ticks, it is believed to be far more widespread than reported statistics indicate. Its etiologic agent is Rickettsia siberica. Known as well as North Asian tick-typhus, this disease is also found in China and in other north Asian republics.
Queensland tick-typhus, caused by Rickettsia australis, was first reported in North Queensland, Australia, in 1946. Its vector tick, Ixodes holocyclus, parasitizes marsupials in addition to wild rodents. In general, people working in forest and scrub areas in northern and southern Queensland are at risk of contracting this disease, although in 1979 an urban focus was reported in Sydney.
The final member of the spotted fever group of diseases is unique in being the only member not transmitted by a tick. Its name, rickettsialpox, clearly reflects its history as a disease defined by the investigators who first studied it. In 1946 a strange disease resembling mild chickenpox and exhibiting an eschar, or initial lesion, was reported in a New York apartment building. Charles Pomerantz, a local exterminator and amateur entomologist, had alerted New York health authorities to the possibility of some sort of arthropod-bome disease after he found mite-infected mice in the apartment-complex basement. New York investigators collaborated with the U.S. Public Health Service, and within 8 months the entire picture of the disease had been elucidated. The etiologic agent of the disease was shown to be a hitherto unknown rickettsia of the spotted fever group. Because the organism was found to inhabit the mite Allodermanyssus sanguineus, a parasite of the house mouse, it was named Rickettsia akari, the species designation meaning “mite.” Epidemiological research determined that the disease was contracted wherever mites had access to human living areas. In the case of the original apartment complex, the mites climbed up a central incinerator and infested the carpeting in apartments, thus rendering young children especially susceptible. In 1949-50 the illness was also identified in the Soviet Union, and was known there as vesicular rickettsiosis. A mild, nonfatal disease, rickettsialpox has not been reported in recent years in the United States and only sporadically in the former Soviet Union.
Victoria A. Harden
Bibliography
Aikawa, Jerry K. 1966. Rocky Mountain spotted fever. Springfield, Ill.
Harden, Victoria A. 1985. Rocky Mountain spotted fever research and the development of the insect vector theory. Bulletin of the History of Medicine 59: 449—66.
1990. Rocky mountain spotted fever: A twentieth-century disease. Baltimore.
Hoogstraal, Harry. 1981. Changing patterns of tickbome diseases in modem society. Annual Reviews of Entomology 26: 75—99.
Lackman, David B. 1963. A review of information of rickettsialpox in the United States. Clinical Pediatrics 2: 296-301.
McDade, Joseph E., and Verne F. Newhouse. 1948. Natural history of rickettsia rickettsii. Annual Review of Microbiology 40: 287—309.
Price, Esther Gaskins. 1948. Fighting spotted fever in the Rockies. Helena, Montana.
Roueche, Berton. 1947. The alerting of Mr. Pomerantz. New Yorker August 30: 28.
U.S. Public Health Service. Centers for Disease Control. 1985. Rocky Mountain spotted fever-United States, 1985. Morbidity and Mortality Weekly Reports 35 (April 18): 247-9.
Wilson, Louis B., and William M. Chowning. 1904. Studies in pyroplasmosis hominis: ‘Spotted fever’ or ‘tick fever’ of the Rocky Mountains. Journal OfInfectious Diseases 1: 31—57.
Woodward, Theodore E., and Elizabeth B. Jackson. 1965. Spotted fever rickettsiae. In Viral and rickettsial infections of man, ed. Frank L. Horsfall, Jr., and Igor Tamm, 1095-129. Philadelphia.