151 Typhus, Epidemic
Epidemic typhus fever is an acute rickettsial disease transmitted among victims by the human body louse, Pediculus humanus corporis. Its characteristic Sjnnptoms include high fever, prostration, headache and body aches, and a widespread rash that covers the trunk and limbs of the body.
Mortality rates in untreated cases vary widely. Broad-spectrum antibiotics provide an effective therapy for the disease.Because of its association with conditions of human misery, typhus has been known by many names. Jail distemper and its variations — morbus carcerum, gaol fever, and jayl fever - indicate the prevalence of typhus in detention facilities. Ship fever, camp fever, and famine fever reflect the poor hygiene characteristic of travel, of military expeditions, and of refugee populations. The characteristic rash of typhus has elicited other descriptive names, including spotted fever in English, Fleckfieber and typhus exanthematicus in German, typhus exanthe- matique in French, tifo exantemdtico and tabardillo in Spanish (the latter meaning “red cloak”), and typhus-esantematico in Italian. Although Hippocrates applied the word typhus, from the Greek word meaning smoky or hazy, to confused or stuporous states of mind frequently associated with high fevers, the word was not associated with the disease as it is currently known until the eighteenth century. After murine typhus was identified, the appellation typhus historique was sometimes applied to the classic, epidemic disease.
Etiology and Epidemiology
Occurring as a natural infection only in humans, epidemic typhus is caused by Rickettsia prowazekii. It is spread from host to host by the human body louse, P. humanus corporis, and less often by the human head louse, Pediculus humanus capitis. The body louse spends its entire existence in the clothes of humans. Eggs laid in the seams of the undergarments hatch after about 8 days, and the nymphs become adults in about 2 weeks, going through three molts.
Each louse takes four to six blood meals a day from its host under natural conditions. Human blood constitutes its only food.Once typhus organisms in infected human blood are ingested by a louse, they multiply rapidly in the cells lining the louse’s intestines and are secreted in the feces of infected lice. Since rickettsiae are not found in other tissues (such as the salivary glands) of the louse, they are transmitted to new human hosts mechanically. This is usually accomplished by contact of infected louse feces with a small abrasion of the skin incurred when the human scratches the unpleasant itch caused by feeding lice. The disease spreads when lice leave feverish or dead victims for new hosts with normal temperatures. Unlike other rickettsial organisms, R. prowazekii is not passed from generation to generation in the eggs of its host arthropod. In fact, as Hans Zinsser of Harvard Medical School pointed out in his 1935 history of typhus fever, humans constitute a great threat to the health and happiness of these small creatures, for humans usually recover from typhus fever, whereas the disease is inevitably deadly for infected lice.
Tjrphus is widely known as a disease of cold climates, appearing in epidemics that usually reach their peaks in late winter and taper off in the spring. This pattern is clearly related to the ideal conditions for multiplication of lice and their rapid transmission to new hosts. Typhus flourishes when people are crowded together in unsanitary surroundings and lack fuel, circumstances that predispose them to wear the same garments day and night for months at a time.
Persons of all ages are susceptible to typhus. Mortality rates in untreated typhus fever vary between 5 and 25 percent, occasionally reaching 40 percent. In children under 15 years of age, however, the disease is generally mild. As age increases, so does mortality.
Clinical Manifestations and Pathology
After an incubation period that may vary from 5 to 15 days, the onset of typhus is abrupt.
Many patients are able to state the exact hour at which they noted the beginning of their illness. Headache, loss of appetite, and general malaise are followed by a rapidly rising fever. Bouts of chills, nausea, and prostration characterize the first week of illness. The most characteristic symptom of typhus is a widespread rash that appears about the fourth to sixth day after onset. Dark, reddish, discrete spots 2 to 5 millimeters in diameter appear scattered over the body and limbs. These lesions at first are bright red, but they rapidly become darker in color and more petechial in character. After recovery, the rash usually fades, but in rare cases it may leave a brownish stain that persists for several months.During the first 2 or 3 days, the fever reaches its maximum, between 102o to 105oF, and is sustained for another 5 days, after which it falls rapidly if the outcome is favorable. In fatal cases, however, prostration becomes more progressive, with neurological symptoms increasing. These may include deafness, stupor, delirium, and eventually coma preceding death. Since 1948, however, when chloramphenicol and the tetracyclines (known collectively as broadspectrum antibiotics) were introduced, no one need die of typhus if diagnosis is made in a timely manner.
Immunology
An attack of typhus confers long immunity. Many children in regions where typhus is frequent may contract Subclinical or mild cases that protect them somewhat from a later, more severe infection. Because R. prowazekii persists in the tissues of its victims even after recovery from the disease, however, symptoms of the disease may reappear years later, especially under conditions of stress when a victim’s immune system is depressed. This phenomenon was noted but not recognized in 1898, when New York physician Nathan Brill described a disease frequently diagnosed as typhoid but having symptoms more closely related to typhus. In 1910 Brill published an exhaustive study of 221 cases, and his thoroughness led to the designation of “Brill’s disease” as a catchall for unknown, typhus-like symptoms.
Two years later, U.S. Public Health Service investigators John F. Anderson and Joseph Goldberger demonstrated reciprocal cross-immunity in monkeys between Brill’s disease and epidemic typhus.For the next two decades, moreover, because of ignorance surrounding many other rickettsial diseases, illnesses exhibiting typhuslike symptoms anywhere in the world were often classified as Brill’s disease. In 1934 Zinsser correctly hypothesized from epidemiological data that Brill’s disease was a recrudescence of epidemic typhus in persons who had earlier suffered an attack of the classic disease. During the 1950s, laboratory investigations confirmed his hypothesis, and the disease was renamed Brill- Zinsser disease.
The first laboratory diagnostic test for typhus grew out of a chance observation in 1916 by Viennese physician Edmund Weil and his English colleague Arthur Felix that a strain of Bacillus proteus was agglutinated by the sera of typhus patients. Later studies revealed that the phenomenon was a chance antigenic “fit,” but the Weil-Felix reaction, as it came to be called, provided a laboratory tool that became useful in several rickettsial diseases. In 1941 a more specific complement-fixation test was developed, and during the 1970s a variety of new techniques have improved the sensitivity and accuracy of laboratory diagnosis.
Distribution and Incidence
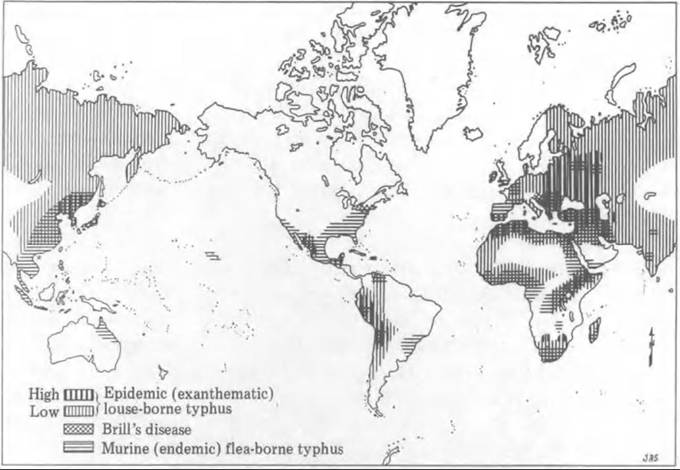
In all areas of the world where public health and sanitation measures have been rigorously enforced, the incidence of typhus has declined dramatically. Cases may erupt in urban slums, and the disease remains a threat to many isolated rural regions. Reporting of cases is poor in many regions of the world where typhus is most prevalent. Map VIIL151.1 shows the worldwide distribution of epidemic typhus during World War II. A recent study indicates that the major areas where typhus-infected lice are widespread have been reduced to three: the Himalayan region of Asia, the Andean regions of South America, and the hom of Africa, especially famine-ridden Ethiopia.
In November 1984, for example, 68 cases were serologically confirmed in one Ethiopian refugee camp. Following treatment with tetracycline antibiotics, however, only three people died. Thus typhus, although causing considerable morbidity, is not at present as great a killer as in past centuries.Map VIII.151.1. Outline map of the world (c. World War II), showing the approximate geographic distribution of epidemic (exanthematic) louse-borne typhus, murine (endemic) flea-bome typhus, and Brill’s disease. (From Stanhope Bayne-Jones, in U.S. Army Medical Department 1964, 177.)
History and Geography
Antiquity Through The Sixteenth Century As a disease having a human reservoir, epidemic typhus has undoubtedly existed for centuries. Although it has been speculated that certain ancient plagues were probably typhus, the first contemporary accounts of a disease that may well have been typhus appeared near the end of the fifteenth century. In 1489-90 during the civil wars of Granada, Spanish physicians described a typhus-like disease that killed 17,000 Spanish soldiers - six times the number killed in combat with the Moors.
In the early sixteenth century, a similar malady appeared in Italy. During the French siege of Naples in 1528, an apparent typhus epidemic may have altered the subsequent course of European history. The French were at the point of decisive victory over the forces of Charles V when the disease appeared and struck down 30,000 French soldiers, forcing the remnants of the army to withdraw. In 1546 Girolamo Fracastoro (Fracastorius), who had observed the epidemics in Italy, published the first clear description of what he termed a “lenticular or punctate or petechial” fever also characterized by headache and general malaise.
In the Balkan regions, where German, Italian, and French troops assembled to combat the Turks, many soldiers were struck by typhus even before they reached the battlefield.
As it was disseminated across Europe by forces returning from Hungary, typhus became known as morbus hungaricus. Toward the end of the sixteenth century, typhus was also recorded in the Mexican highlands, where it killed more than 2 million Amerindians. It remains unclear, however, whether the disease was brought to the New World by Spanish explorers or, as some evidence indicates, was known to the Aztecs and some pre-Columbian Indians in Mexico.Early to Mid-Nineteenth Century
Typhus increased dramatically in the early nineteenth century. In 1812 Napoleon’s catastrophic expedition to Russia was plagued by typhus. Between 1816 and 1819, moreover, a great epidemic of the disease struck 700,000 people in Ireland, whose population was only 6 million. For several decades, however, confusion characterized medical understanding of the disease. By the late eighteenth century, the medical nosologist Boissier de Sauvages had begun using the word typhus to describe the neurological symptoms of typhus, but few attempts were made to distinguish pathologically between typhus and typhoid fever, which also produced a red rash. Even into the twentieth century, confusion between typhoid and typhus was perpetuated in the nomenclature. In many European countries, the former was known as typhus abdominalis and the latter as typhus exanthematicus.
In 1837 Philadelphia physician William Wood Gerhard, who had studied the distinctive intestinal lesions of typhoid as a student of Pierre Louis in Paris, noted their absence in victims of typhus fever, which had been epidemic in Philadelphia the previous year. Gerhard’s work, however, was not immediately embraced by physicians who clung to older theories of the unity of fevers. It was not until mid-century that additional pathological and epidemiological research, especially by William Jenner and Austin Flint, convinced most American physicians that typhus and typhoid were distinct disease entities.
The European revolutions of 1848 spawned typhus epidemics in eastern Europe, as did warfare in Ethiopia. During a particularly severe typhus epidemic in Upper Silesia, the German physician and politician Rudolph Virchow published a radical assessment of the epidemic that subsequently cost him his government post. Observing that the disease afflicted the poor, the uneducated, and the unclean, Virchow called for democracy, education, and public health measures as the proper “treatment” of the epidemic.
Late Nineteenth Century Through World War I Although typhus itself subsided during the latter half of the nineteenth century, the advent of the germ theory of disease during the 1870s spurred bacteriologists to search for a microbial cause for the classic scourge. In 1909, exploiting recent discoveries about the role of insect and other arthropod vectors of microorganisms, Charles Nicolle, director of the Institut Pasteur in Tunis, North Africa, demonstrated that the body louse was the vector of typhus. The following year, Howard Taylor Ricketts, who was investigating typhus in Mexico City, described small bacteria he found in the blood of typhus victims, in infected lice, and in lice feces. Before Ricketts could confirm his observations, he contracted typhus and died. In 1916 the Brazilian Henrique da Rocha Lima described similar organisms, which he named Rickettsia prowazekii, the genus name after Ricketts and the species name after Polish researcher Stanislaus von Prowazek, who had also died from a laboratory-acquired typhus infection.
During World War I, military forces on both sides of the conflict acted on Nicolle’s discovery, instituting delousing procedures to combat typhus. These included bathing and steam-treating clothing to kill lice. Among poor civilian populations in war-tom eastern Europe, where such preventive measures were not enforced, the disease continued to exact a high rate of mortality. In 1915 Serbia was particularly hard hit, and typhus settled with a vengeance on Russia and Poland after 1918. Typhus research in Poland after World War I, sponsored by the League of Red Cross Societies, confirmed Rocha Lima’s assertion that R. prowazekii was the cause of typhus. Even so, because rickettsiae could not be cultured on lifeless media like ordinary bacteria, their etiologic relationship to typhus and other rickettsial diseases was not firmly established until the late 1930s.
Postwar Period Through World War II
During the 1920s and 1930s, empirical research on a vaccine against typhus was hampered because the organisms could not be grown in necessary quantities outside of living cells. Displaying ingenuity in the face of this limitation, researchers prepared vaccines from infected lice intestines, from lice feces, and from the typhus-infected lungs of rats. Then in 1937 U.S. Public Health Service investigator Herald R. Cox discovered that rickettsiae grew luxuriously in the yolksacs of fertile hens’ eggs. This method simplified vaccine production and made it commercially feasible just as the onset of World War II again raised concern about large-scale typhus epidemics.
The threat of typhus was a key factor in Allied military plans during World War II, and in 1942 President Franklin D. Roosevelt created an extraordinary body, the U.S.A. Typhus Commission, to combat typhus wherever it might threaten the U.S. military efforts. The so-called Cox vaccine was administered to all Allied military personnel, and although experience during the hostilities indicated that it did not actually prevent the disease, it clearly ameliorated its course. Intensive research on antilouse agents by government and private groups, moreover, demonstrated that lice could be effectively controlled by dichlorodiphenyl-trichloroethane, more commonly called DDT. This powder could be applied with a “blowing machine” to puff it under clothes without their owners having to remove them. The method was not only faster, it was also accepted by even the most modest civilians. DDT also proved to be highly effective in the typhus epidemic that occurred during the winter of 1943-4 in Naples, Italy. With astonishing rapidity, the nascent epidemic collapsed. Within two decades, however, the ability of lice to become resistant to DDT had been documented. In addition, the chemical’s ecological hazards were found unacceptable, and it is no longer widely used to prevent typhus.
Prophylaxis and control of typhus with the Cox vaccine and with DDT during World War ∏ reduced typhus from a major threat to a mere nuisance among Allied troops. Only 104 cases occurred among U.S. military personnel, with no deaths. In contrast, severe epidemics occurred among civilians in North Africa, Yugoslavia, the German concentration camps, Japan, and Korea.
Mid-Twentieth Century to Present
In 1948 the tetracyclines and chloramphenicol, known together as broad-spectrum antibiotics, were discovered to be effective treatments for rickettsial diseases. Since the late 1940s, efforts to combat typhus have depended almost exclusively on these antibiotics. In 1980 concern about the limited efficacy and side effects of the Cox vaccine halted its production, and at the present writing, no typhus vaccine is commercially available. Recent research, moreover, has indicated that the humoral immunity stimulated by all existing rickettsial vaccines is less important than is cell-mediated immunity. At present, genetic engineering techniques are being employed in research on a more effective vaccine.
Since 1950, typhus has been reported most frequently from the horn of Africa, from the high plains of the Andes in South America, and from the Himalayan regions of Asia - all areas characterized by rural poverty and cold weather. In one survey of Bolivian army recruits, for example, 80 percent had antibodies against the disease. Another study in a Bolivian village near the Peruvian border found mild typhus in children often confused with measles. Typically, the disease was more severe in afflicted adults than in children.
In Ethiopia, with its frequent famines, thousands of cases of typhus have been documented in recent years, especially in refugee camps. Similar ecological and sociological conditions in neighboring countries suggest that the disease may also be widespread in them but masked by poor reporting. Reliable statistics are also virtually impossible to obtain from the Himalayan regions of Asia.
Since Nicolle’s identification of the body louse as the vector of typhus, the slogan “no lice, no typhus” has been the watchword of public health efforts against this disease. But as Hans Zinsser noted in 1935, typhus will always remain a smoldering threat, ready to break out at any time that war, famine, or other catastrophes remove the public health barriers against it.
Victoria A. Harden
Bibliography
Anderson, John F., and Joseph Goldberger. 1912. The relation of so-called Brill’s disease to typhus fever. Public Health Reports 27: 149—60.
Brill, Nathan E. 1910. An acute infectious disease of unknown origin: A clinical study based on 221 cases. American Journal of Medical Science 139: 484—502.
Edlinger, E. 1986. Actuality des Rickettsioses. Archives de VInstitut Pasteur de Tunis 63: 75—90.
Fracastoro, Girolamo. 1589. De morbis contagious. In Opera omnia. Venice.
Gear, J. H. S. 1984. Studies of the rickettsial diseases at the South African Institute for Medical Research: Epidemic louse-bome typhus fever. Adler Museum Bulletin 10: 8-15.
Gerhard, William Wood. 1837. On the typhus fever, which occurred at Philadelphia in the spring and summer of 1836. American Journal of Medical Science 19: 289— 92, 298-9, 302-3.
Loeffler, W., and H. Mooser. 1952. Ein weiterer Fall von Brill-Zinsserscher Krankheit in Zurich (Spater Riick- fall bei klassischem Fleckfieber). Schweizer Medizin- ische Wochenschrift 82: 493.
Pankhurst, Richard. 1976. Some notes for the history of typhus in Ethiopia. Medical History 20: 384-93.
Smith, Dale C. 1980. Gerhard’s distinction between typhoid and typhus and its reception in America, 18331860. Bulletin of the History of Medicine 54: 368-85.
Snyder, John C. 1965. Typhus fever rickettsiae. In Viral and rickettsial infections of man, 4th edition, ed. Frank L. Horsfall, Jr., and Igor Tamm, 1059-94. Philadelphia.
U.S. Army. Medical Department. 1964. Preventive medicine in World War H, Vol. 7: Communicable diseases: Arthropodborne diseases other than malaria. Washington, D.C.
Virchow, Rudolf. 1985. Report on the typhus epidemic in Upper Silesia. English trans. In Rudolf Virchow: Collected essays on public health and epidemiology, 2 vols., ed. L. J. Rather, Vol. 2, 205-319. Canton, Mass.
Zinsser, Hans. 1934. Varieties of typhus virus and the epidemiology of the American form of European typhus fever (Brill’s disease). American Journal of Hygiene 20: 513-32.
1935. Rats, lice and history. Boston.