Bioarchaeological data and the transition to agriculture
While many studies of the agricultural transition using skeletal remains have found a decline in health, not all studies follow that trend, which suggests that the association is not so easy to understand at first sight.
It is therefore instructive to now take a closer look at the indicators that most scholars use to assess health and how a change in any one health indicator can be interpreted in different ways.In exploring the impact of economically based transitions such as that to agriculture, bioarchaeologists consider a wide range of ‘markers' on the bones and teeth of skeletons that are accepted as indicating ill health, and also changes in the shape and size of bones and teeth. It should be stated at the outset that interpretation of these observations is challenging because these normal and abnormal variations may often be attributable to more than one cause. As discussed above, the quality of diet impacts the strength of the immune system, and consequently health. Therefore, evidence of dietarydeficiency-related diseases, and also diseases that are related to the consequences of living in settled communities, are relevant to questions about diet and health in pre- and post-agricultural contexts.
Bearing in mind that abnormal (disease) variation may have both environmental causes, in their widest sense, but also a genetic predisposition, it is sensible to divide the subsistence-related markers of ‘normal' and ‘abnormal' variation into those specifically related to diet, those related to the ‘living environment', and ones that cover both themes. Dental caries, calculus, and attrition, scurvy (vitamin C deficiency), and changes in

Figure 4.3 Dental caries in first permanent molar tooth.
craniofacial morphology and tooth size (‘shape/size change') are specifically relevant to dietary deficiencies and excess.
Specific (e.g. bacterial) and non-specific (e.g. respiratory) infections, possible work-related conditions (e.g. trauma, entheseal changes, changes in biomechanical properties of bones, joint degeneration), and injuries related to conflict are relevant to living conditions. Both themes may also be characterized by specific demographic profiles, growth retardation (long bone length and attained stature, Harris lines of arrested growth), enamel hypoplasia, cribra orbitalia, and porotic hyperostosis.Diet: skeletal changes
Dental caries (destruction of the tooth structure) results from an oral environment that is acidic, caused by fermentation of carbohydrates, especially sugars, by bacteria in plaque (Figure 4.3). Sugars in other foods, beyond starchy cereals/domesticated plants, may also cause caries, for example honey and fruit. Caries has been documented to increase in farmers compared to huntergatherers in many studies, but this is not a consistent pattern. For example, in the Levant, dental caries rates were similar in Natufian hunter-gatherer people compared to the Neolithic.[172] A further example shows that rice agriculture is apparently not as likely to cause caries as other cereals: in Southeast Asia Tayles et al. found caries did not increase with the adoption of rice agriculture.[173] More recent work also shows no decline in infant dental health with intensification of rice agriculture.[174] Temple and Larsen, furthermore, found no real difference in caries rates between hunter-gatherers and agriculturalists in prehistoric Japan (Jomon and Yayoi, respectively).[175] They suggested that rice was no more cariogenic than other carbohydrate foods consumed by the Jomon. Females in general suffered caries more than men and, with the transition to agriculture, this difference intensifies, being attributed to increased demands on women due to increased fertility.[176]
Of course, extreme dental wear will expose the dentine underlying the enamel and the tooth pulp cavity, predisposing the tooth to caries (and dental abscess), and possible antemortem tooth loss.
Dental attrition or wear differs in character from flat (hunter-gatherer) to angled (agriculturalists) but, overall, dental macro- and microwear generally decline with agriculture due to the softer nature of foodstuffs being eaten. However, individual microwear features have been shown to change from the Mesolithic to Neolithic periods. Intensification of agriculture further leads to increased dental disease. Inflammation of the gums (gingivitis) as a result of plaque buildup, and subsequent periodontal disease (inflammation and loss of bone in the jaws), are also exacerbated by the softer carbohydrate foods of a farming community. Dental calculus (calcified plaque) is generally seen in people eating a high protein diet, and thus would be expected to be seen more in hunter-gatherer populations. Unfortunately many studies of the agricultural transition have not systematically recorded calculus, until recently. It is clear, however, that calculus on teeth of archaeological skeletons tends to be ubiquitous regardless of subsistence economy.[177] In recent years dental calculus has been examined in much more detail, in light of developments in biomolecular methods, and these studies have much potential for exploring oral ecology at the transition to agriculture. For example, Adler et al. document a change in the oral flora at the transition to agriculture, albeit with a small sample size.[178] The fact that dental calculus is a common finding on all skeletal remains, and that pathogenic aDNA has now been isolated from it, indicates the potential for its use in answering questions about the past, not only concerning the agriculture transition.Deficiencies of dietary constituents as a result of agriculture include a range of conditions, some of which can be identified in the skeleton. For example, vitamin C is necessary to absorb iron, so iron deficiency often occurs along with scurvy (vitamin C deficiency), and cereals contain no C, creating the potential for C deficiency.
Recognized primarily by a specific patterning of new bone formation reflecting a response to haemorrhaging fragile blood vessels, systematic studies of scurvy in pre- and post-agricultural populations have not yet been done, probably because the diagnostic criteria for skeletons have only fairly recently been published, and many of the synthetic studies on health and the transition to farming were done many years before the late 1990s.[179] Even so, there is little reference to scurvy in Cohen and Crane-Kramer, suggesting that most authors either did not record it, misdiagnosed it, or it was not present.[180] Of course, fresh fruit and vegetables are essential to prevent scurvy and one might imagine that practising agriculture could have led to a decline in their consumption in a less varied diet. Another response of the skeleton to a deficiency in diet is that of osteopenia and subsequent osteoporosis (low bone density), resulting from calcium deficiency. Cereals are a poor calcium source and cereal phytates affect its absorption (as seen for iron).[181] It would be expected, therefore, that these conditions would rise in frequency with the agricultural transition, and a reduction in ‘activity' when compared to hunter-gatherers would exacerbate the problem. Osteoporosis is diagnosed in a number of ways, including thinning of the cortical (outer layer) bone, reduced bone mass as seen in the trabecular honeycomb (internal) structure, and fractures of the hip, wrist, and spine; a decline in cortical thickness has been found in a number of studies, but diagenesis (post mortem damage) can compromise diagnosis.[182]Other nutrient deficiencies may also be considered but may or may not be recognized in the skeleton. These include protein deficiency, seen for example in maize, rice, and wheat agriculture, which can lead to growth retardation, as can low zinc levels with wheat consumption.
Pellagra (low niacin or vitamin B3) can also occur and is related to maize agriculture. Periodontal disease (non-specific infection), dental caries, enamel hypoplasia, periosteal new bone, osteomyelitis, cribra orbitalia, and cranial pitting have been described as a suite of features associated with this condition.[183] In this study of skeletons representing people with a known diagnosis of pellagra, and people who had general malnutrition at the time of death, in the Raymond Dart twentieth-century documented skeletal collection of South Africans, the frequency of this suite of indicators separated the pellagrous from those with non-specific general malnutrition, but the indicators were not pellagra specific. Finally, and something that will be discussed further below, cribra orbitalia and porotic hyperostosis (porosity in the eye sockets - Figure 4.4 - and on the skull vault, respectively), which appear to rise in frequency with the transition to agriculture, have also been long been associated with iron deficiency as a result of a reliance on low-iron-content cereal crops and inherent phytates.[184] However, ideas have changed as to what causes the bone changes of cribra orbitalia and porotic hyperostosis.Changes in craniofacial shape (morphology) and tooth size are fairly consistently shown in studies of crania of hunter-gatherers and agriculturalists; the shape of skulls changes and robusticity declines, along with a reduction in jaw and tooth size and crowding of teeth. These changes are again due to the softer nature of the agricultural diet and reflect less demand on the chewing muscles. People who hunted and gathered had long and narrow skulls and those practising farming had shorter and wider skulls,[185] and this suggests that jaws got smaller and could not accommodate the teeth without recourse to crowding and size reduction. An extensive study of tooth size in over 600 individuals, dating from the early upper Palaeolithic to the late Neolithic

Figure 4.4 Cribra orbitalia in orbit.
across central Europe, found a trend through time to tooth reduction into the early Neolithic, but in the Levant the reduction was much more severe (up to twelve times higher). It was concluded that dental size changes should always be interpreted on an individual basis according to region.[186] Teeth are under genetic control, suggesting tooth size reduction is an evolutionary change, but that under stressful conditions, such as when agriculture was adopted, teeth failed to reach their genetic size potential. This illustrates the importance of considering both genetic and environmental causes for observations of biological changes.
The identification of the type of diet people were eating is also increasingly being accessed through stable isotope analysis. Here carbon and nitrogen isotope values are analysed in teeth and bone to assess the overall components of the diet, for example the relative proportions of marine versus terrestrial resources.[187] Diet at the transition to agriculture has been a large focus of the work to date. For example, Lillie and Richards studied skeletons from late Mesolithic/early Neolithic Ukraine (10,000-4500 cal bce) and found people were eating a hunter-fisher-gatherer diet throughout, with increased fish consumption into the Neolithic period.[188] However, Lubell et al. in their study of Mesolithic and Neolithic sites in western central Portugal (7,240 ± 70 bp to 4,110 ± 60 bp) found that people ate terrestrial and marine foods in the Mesolithic but only terrestrial foods in the Neolithic.[189] It is clear from many studies that the Mesolithic-Neolithic transition in Europe was not a ‘one size fits all' situation in terms of stable isotope analyses and skeletal indicators of normal and abnormal variation - there was much variation at the transition to agriculture, remembering that individual people and populations can react differently to the same ‘events', as they do today.[190]
Living environment: skeletal changes
While dietary-related observations of skeletal remains are important for consideration in a world with agriculture, the changes people experienced in how they lived their daily lives are also reflected in their skeletons. The health indicators here relate to poor air quality, population density increases, living with animals, and working on the land. Firstly, respiratory disease (sinus and lung inflammation as a result of infection, allergies, indoor pollution, etc.) maybe recognized in facial sinuses and on ribs (Figure 4.5), but it is only recently that scholars have focused on these bones in human remains. This means that it is difficult to assess how common poor air quality was pre- and post-agriculture. However, in a study of a range of hunter-gatherer, rural agriculture and urban populations from North America, England, and Sudan, hunter-gatherers had less sinusitis than rural agriculturalists and urban populations, suggesting hunter-gatherers were exposed to better quality air.[191] Studies of farming communities have also found evidence for respiratory disease, this time on ribs. However, it is important to recognize that rib lesions may be caused by many lung conditions, and until systematic studies of these bone changes are undertaken it is impossible to assess more widely their frequency in hunter-gatherers compared to agriculturalists.
Infections generally need high population numbers and density to enable spread from human to human and then maintain them in the population. At the advent of agriculture, as populations increased, this provided ideal conditions for infection, along with humans living side by side with their animals, often in
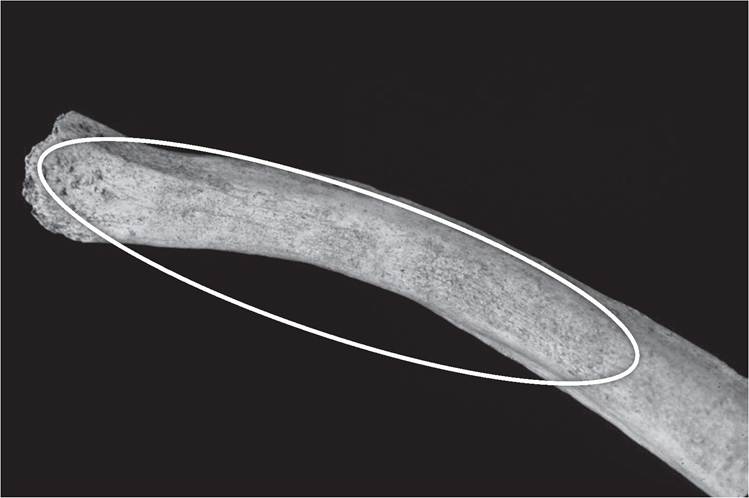
Figure 4.5 Rib with new bone formation on it.
the same living quarters. Depressed immune systems (due to poor quality foods) and poorer living conditions also contributed to make people more susceptible to infectious disease. Specificbacterial infections such as TB (destruction of the spine) are seen to rise with farming, which could be related to both an increasing population density, allowing respiratory droplet spread of the infection from human to human, but also closer contact with tuberculous animals and ingestion of their products.[192] Another bacterial infection, also affecting the spine, but only caught from animals, is brucellosis, which would also be expected in farming communities in the past but, as yet, few reports of evidence in skeletons have been made. However, although these two infections can affect a range of domesticated animals, they can also be seen in wild animals, thus having the potential to infect humans via hunting and butchery activities (although they have generally not been reported in hunter-gatherer populations). The potential threat of zoonoses being transmitted to humans in both hunter-gatherer and agricultural populations is as yet unknown because of the lack of work on the zoonoses in archaeozoology.[193]
Possible work-related conditions have been a focus of studies of health in farmers. Physical activity can ultimately have an impact on bone, and this

Figure 4.6 Normal vertebra (left) and one with a healed fracture to the spinous process (‘clay-shoveller’s fracture').
may be seen in a change in size and/or shape,[194] reflecting increasing robus- ticity. Additionally, entheseal changes, i.e. new bone formation or destruction at muscle, tendon, and ligament attachment sites on bones, degeneration of joints (osteoarthritis), and specific fractures, e.g. of the fifth lumbar vertebra (spondylolysis), and of the spinous process of the lower cervical or neck vertebrae (‘clay-shoveller’s fracture’, Figure 4.6), may also reflect ‘activity’. It should be noted that all these bone changes could have other causes beyond physical activity, for example increasing age causes osteoarthritis and entheseal changes (Figure 4.7).[195] Indeed, much discussion has centred on whether it is possible to infer ‘occupation’ from these bone changes, and scholars have even found non-correlation of skeletal markers with heavy and light manual occupations.[196] Indeed, a recent study of a historically dated skeletal remains from rural agricultural Yorkshire, England, found recorded occupation at the time of death is insufficient to aid in interpretation of entheseal changes.[197] Recent work has highlighted that

Figure 4.7 Entheseal changes (new bone formation in form of a spur) to end of ulna (forearm bone).
‘There are clear problems relating methodology between EC [entheseal changes], occupation and biomechanics'.[198]
With respect to bone size and shape, hunter-gatherers tend to have more robust bones and prominent muscle attachment sites, and some studies show more circular cross-sections in bones of agriculturalists, reflecting mechanical factors related to greater physical activity in foragers and a reduction in farmers. Logically the frequency of entheseal changes and osteoarthritis would be expected to decline with the adoption of a more sedentary life, such as the adoption of agriculture, and they do, with exceptions which likely reflect local and regional terrain effects.[199] Bridges noted in her study of hunter-gatherers and agriculturalists in Alabama that the former had more osteoarthritis but that differences were not significant statistically.[200] As an extension to this discussion, there are ‘activity'-related non-metric traits (Figure 4.8), but it is very challenging indeed to determine whether activity led to the traits or produced an ‘environment' conducive to trait development. Using all these kinds of ‘bone markers' to assess ‘activity' at the transition to farming is fraught with problems, and published data - and interpretations thereof - should not be considered lightly. However, many scholars are now working towards improving recording methods and interpretive tools to better nuance these kinds of data.
Injuries related to accident and conflict at the transition to agriculture also show a mix of rises and declines.[201] While hunter-gatherer populations do show evidence of interpersonal violence, this evidence increases for some groups with the adoption of agriculture, suggesting competition over land.[202] However, the evidence is not consistent. For example, in a study of interpersonal violence at four sites on the Danube (Mesolithic and Neolithic Serbia-Romania), Roksandic et al. found no evidence of an increase in interpersonal violence in the Neolithic.[203] With regard to accidental injuries as a result of daily living, it might be expected that different types of fracture might be experienced by hunter-gatherers and agriculturalists (and vary according to terrain and ‘activity'). Indeed, Judd and Roberts found a range of bones fractured in people associated with a medieval farming village in England, with a higher frequency overall when compared to urban

Figure 4.8 Femur (thigh bone) with circumscribed area of destruction (Allen's fossa), possibly related to ‘activity'.
populations.[204] Using ethnographic analogy, different possible ‘occupations' associated with farming were explored here as potential causes.
Diet and living environment: skeletal changes
When it comes to skeletal changes potentially reflecting both diet and living environment, demographic profiles, growth retardation, and cribra orbitalia and porotic hyperostosis are relevant. Chamberlain notes that sedentary populations can sustain high fertility rates and, with the adoption of farming, those higher fertility rates are indeed seen, with peak fertility at an earlier age.[205] Reasons for increased fertility include the reduced need to carry dependent offspring around, in contrast to the case for hunter-gatherers, and the fact that food supply increases, and there is a ready availability of weaning foods, and better food security. It has also been shown that people who adopted farming had lower mean ages at death than hunter-gatherers. Growth retardation may be reflected in reduced long bone length when compared to dental age in non-adult skeletons (i.e. bones shorter than they should be for the age of the person), smaller attained stature in adults, Harris lines of arrested growth, and enamel hypoplasia. As there are problems with recording and interpreting Harris lines, including differences in the number of lines counted by different observers but also by the same observer (inter- and intra-observer error), they are not discussed further.
In effect, because farming communities appear to have had poorer diets than their hunter-gatherer forebears, it is therefore not surprising that growth problems are seen to increase with agriculture. Studies in Cohen and Armelagos and Cohen and Crane-Kramer consistently report declines in stature and juvenile growth rates, and increases in enamel hypoplasia, cribra orbitalia, and porotic hyperostosis with agriculture, and later intensification.[206] However, while Meiklejohn and Babb, in their study of stature and long bone length in 68 upper Palaeolithic, 173 Mesolithic, and 467 Neolithic individuals from Europe, found a decline in long bone length from early to late upper Palaeolithic Europe, they detected no change from the late Palaeolithic through to the Neolithic.[207]
Enamel hypoplasia (Figure 4.9), defects in tooth enamel that reflect disruption to the normal growth of the enamel prenatally and in early childhood, has been recorded as correlating with reduced longevity and also caries susceptibility.[208] The former probably accords with the developmental origins hypothesis of Barker.[209] They furthermore have been seen to correlate with infection in the same individual. Enamel hypoplasia has been associated with dietary deficiency and many childhood diseases, but the former cause is considered dominant. Increases in enamel defects have been noted by many with the transition to agriculture. For example, in early
18" class="lazyload" data-src="/files/uch_group31/uch_pgroup24/uch_uch7223/image/image017.jpg">
Figure 4.9 Enamel hypoplasia in teeth (lines/grooves).
agricultural Egypt and Nubia enamel hypoplasia was greatest in pastoralist communities but declined with state formation, increased urbanism, and trade.[210] A study of enamel hypoplasia in India has focused on the impact of climatic deterioration on frequency rates, the deterioration having caused a move back to nomadism from farming.[211] Frequency rates declined with this transition, and these were interpreted as indicating a more diverse and protein rich diet, with consequently less physiological stress.
Cribra orbitalia and porotic hyperostosis, as has been discussed above, have long been reported as having higher frequencies in people practising agriculture compared to hunter-gatherer, and as being related to iron deficiency anaemia. However, now these lesions are seen as having a more complex aetiology, suggesting megaloblastic (e.g. caused by a deficiency of vitamin B12, found in high quantities in liver, eggs, shellfish, fish, beef, lamb, and cheese) or haemolytic anaemias such as sickle-cell anaemia and thalassaemia.[212] Iron-poor foods (including cereals) or foods containing phytates (maize and wheat) that inhibit iron absorption, but also high pathogen loads (infection), including parasitic infections, are also believed to be key to development of cribra orbitalia/ porotic hyperostosis.[213] Indeed, infection actually leads the body to withhold iron and make itself iron deficient to prevent pathogens surviving in the body. It has been suggested that while increased pathogen loads can lead to iron deficiency, conversely iron deficiency can prove protective against infection (e.g. in children). Research has also illustrated the synergistic relationship between nutrition and health. In a study that focused on the influence of iron and protein on TB bone changes, it was concluded that these two dietary components could influence whether TB caused bone changes that would be visible in the skeleton.[214] Indeed, there is a strong association between how a bone functions, or does not, and a person's immune system status, which clearly has implications for which abnormalities are visible in skeletal remains and their subsequent interpretations.[215] The association of cribra orbitalia and porotic hyperostosis with the haemolytic (or genetic) anaemias appears to be an adaptive response to malaria. It is highly likely that the occurrence of porotic hyperostosis and cribra orbitalia in studies in some regions of the world will relate to malaria, and it is well known that land clearance for farming, permanent settlements, and stagnant pools of water all allow malarial mosquitoes to flourish.
It should be emphasized that while the suite of ‘skeletal markers' recorded to assess diet and health with the transition to agriculture described above is extensive, some scholars concentrate on documenting frequency rates for a smaller subset of these markers, and some diseases are not really considered at all (e.g. the rarer developmental problems, i.e. abnormalities people are born with, and neoplastic conditions (tumours) that can have both genetic and environmental causes).