Bioarchaeology: principles, methods, and data
Principles
First, it is imperative that the workings of ‘bioarchaeology' are outlined. Bioarchaeology, in the US sense, is the study of human remains, whether they are skeletons (inhumation or cremation burials) or preserved bodies.
It is a subdiscipline of archaeology and of physical or biological anthropology, both of which are subfields of anthropology. It encompasses the study of individual skeletons or preserved bodies, and ‘populations' of skeletons (or bodies) from all periods of time, and all areas of the world, although the amount of work in this field can be variable across time and space. This depends on many factors, not least whether there is a tradition in bioarchaeology and whether training is available.[140] Likewise some parts of the world preserve human remains better than others (for example, the very cold or dry areas preserve complete bodies), and some funerary rituals can enhance(e.g. burial in crypts inside coffins) or compromise (e.g. burial in acidic soils) the survival of the evidence that is ultimately excavated and analysed. This chapter will focus on the study of skeletal remains, because this is the most common type studied in bioarchaeology.
Methods and data
Bioarchaeological studies collect a range of data from skeletons from an array of different funerary contexts; the data include primarily the minimum number of individuals represented, the biological sex of the adult skeletons, age at death of both adults and non-adults, and normal (measurements and non-metric traits) and abnormal (disease) variation.[141] In order to understand differences in responses to sociocultural, economic, and political changes in the past using these variables, comparative analyses are done between ‘populations' of the same and different time periods and geographic locations.
Of note, however, is that not all scholars record the same parameters for skeletons they are studying. This can make comparative analyses impossible.[142]While the variables described above are collected ‘macroscopically' (observation with the naked eye), analytical methods have become more sophisticated, especially in recent years, particularly with the application of stable isotope analysis to answer questions about diet and mobility and ancient DNA analysis to consider disease diagnosis and evolution, relationships between people, and migration.[143] These methods have developed alongside improvements in imaging techniques and histological analysis which have all allowed a nuancing of data previously not possible.[144] Established methods for data collection are recommended and, in the main, are used, and many studies are hypothesis and/or question driven.[145] Most importantly, the data from human remains are always (or should be) placed in context. Understanding the archaeological context from which the remains derive is essential for interpretation: this multi-method, multidisciplinary approach to bioarchaeolo- gical studies ultimately aims to generate the 'best fit' interpretation for the data collected.[146]
Normal variation (age, sex, metrical and non-metrical analysis)
Always in the background to such studies is the cautionary approach to interpreting collected data, particularly that relating to health indicators.[147] Additionally, methods may not necessarily be well developed and can have limitations, and one question that always plagues bioarchaeology is whether the population being studied is representative of the living population. It is also not possible to biologically sex non-adult skeletons with any accuracy, although it is more straightforward for adults, depending on completeness of the skeleton.
However, ancient DNA analysis can help if the aDNA is preserved in the skeleton.[148] Conversely, assessing age at death of non-adult skeletons using dental development and bone growth produces relatively accurate ages, while for adults the methods available can overage young adults and underage older adults.[149] However, these problems are being addressed by new research, and one hopes that in the future we will have easy to use and reliable methods to place skeletons into age categories beyond ‘50 years+'. Skeletons are often fragmentary and can be poorly preserved, reflecting the vagaries of different ways of ‘disposing' of the dead over time, and regions which enhance or compromise preservation. This affects not only whether it is possible to age and sex a skeleton but also whether ‘normal variation' can be recorded via measurements of bones and teeth and recording of non-metric traits.[150] Comparisons of data between populations allow bioarchaeologists to explore differences in size and shape of bones and teeth, including, for example, height as determined from long bone length (stature). It may also be possible to say whether people have a high frequency of inherited ‘traits' that either identify them as locally born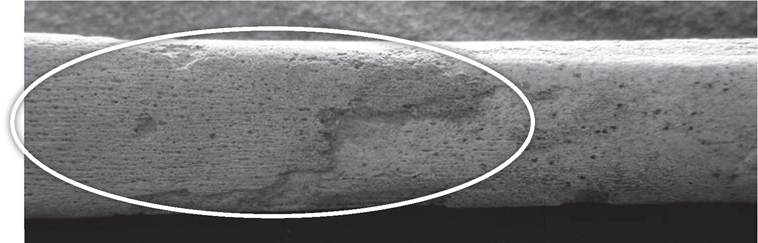
Figure 4.1 Example of bone formation on tibia (lower leg bone).
and raised or highlight them as non-locals with bones and teeth of different sizes and shapes, along with non-metric traits that are not commonly found in the local population. This can of course now be tested using stable isotope analysis.[151]
Abnormal variation (palaeopathology)
The final class of data collected from skeletons is that which indicates health problems experienced during life. Notwithstanding the limitations to these data, discussed below, it has to be remembered that the health indicators recorded reflect those diseases and traumas experienced over the whole course of a person's life.
They are imprinted on the person's bones and teeth as bone formation and destruction, and loss of bone and/or dental tissue in the jaws (Figures 4.1 and 4.2). However, the skeletons of only a small percentage of people will necessarily be affected by disease and trauma because so many diseases (and traumas) affect only the soft tissues of the body. Even diseases that do affect the skeleton may only damage a few per cent of people; for example, the infectious diseases tuberculosis and leprosy only affect 3-5 per cent of untreated people. More often than not when a disease is seen in bones the changes are chronic and healed, indicating a longstanding problem, and the fact that the person survived the acute stages of the disease and did not die from it (strong immune system): they are essentially the ‘healthy ones'.26Once the bone changes are recorded, their distribution pattern is examined and compared to clinical data, and possible differential diagnoses are produced. For example, destructive lesions of the spine can occur in tuberculosis, osteoporosis, cancer, fungal diseases, and brucellosis, but their characteristics (and whether there is any other corroborative bone change elsewhere in the
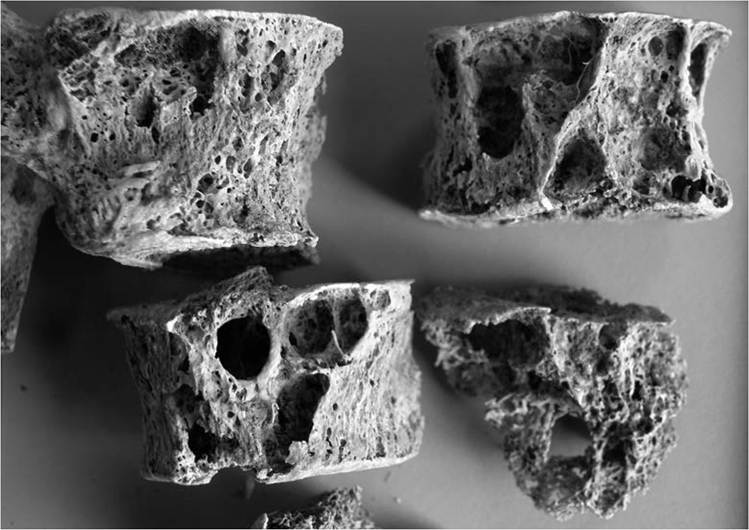
Figure 4.2 Example of bone destruction in vertebrae.
skeleton) will help narrow down the diagnosis. Radiography, histology, and aDNA analysis may help with diagnoses, although they must not be seen as the ‘silver bullet'! It should be noted that the skeleton of a person who died of an acute disease will look very similar to that of someone who did not have the disease.[152] Using clinical data it is also possible to map signs and symptoms onto diseases that are recognized in skeletal remains, such that it is possible to build up a hypothetical picture of the ‘disease experience' of the individual. However, individuals can react differently to the same disease and not necessarily have the same suite of symptoms. Frequency data are produced for the different disease ‘categories' (e.g. infectious, dental, metabolic), and those frequencies compared by age and sex categories, as appropriate and where possible. There may also be comparisons between social statuses and populations of the same or different time periods and geographic regions. Increasingly, the health of our ancestors is considered thematically so that it is possible to explore the effects of living conditions, diet and economy, work, trade, mobility, and access to health care on their experience of disease and trauma. Essentially, bioarchaeological studies of health and well-being provide a deep-time perspective on understanding the origin, evolution, and history of disease, which is very relevant to the emerging discipline of evolutionary medicine.