46 Encephalitis Lethargica
Foremost among recorded encephalitis epidemics was the global pandemic of encephalitis Iethargica that emerged in and from Europe during the last years of the Great War and occurred in successive waves throughout the world during the following decade.
Although the diagnosis of encephalitis lethargica is sometimes applied to sporadically occurring cases of inflammation of the brain having a strong lethargic or stuporous aspect, this discussion focuses upon the encephalitis pandemic that accompanied and followed the 1918 influenza pandemic.Clinical Manifestations and Pathology
Clinically, encephalitis Iethargica was characterized by diffuse involvement of the brain and spinal cord, producing practically the entire range of the signs and symptoms of neurological disease. Sometimes occurring in close conjunction with respiratory- spread influenza, but more often after a long interval, encephalitis patients developed an illness usually characterized by the triad signs of fever, lethargy, and disturbances of eye movement, along with a broad range of other signs and symptoms. These included headache, tremor, weakness, depression, delirium, convulsions, the inability to articulate ideas, coordinate movements, or recognize the importance of sensory stimuli, as well as psychosis and stupor. Oculogyric crisis (eyeballs fixed in one position for a period of time) and other disorders of eye movement, the most frequent sign of localized damage to the nervous system, were present in three-fourths of the cases. Lethargy, another common symptom, in some patients lasted only a few days, but in others it persisted for weeks and months or until death from comatose respiratory failure. Not infrequently, spasmodic twitching and severe psychic and behavior changes persisted long after the acute illness. Approximately a third of encephalitis Iethargica patients died of their acute illness, and a large proportion (80 percent) of survivors developed parkinsonism during ensuing decades.
The main pathological findings during the acute encephalitic illness were a diffuse inflammatory reaction in the meninges and around the blood vessels of the brain and the spinal cord; degenerative changes were found in the neurones, especially in the brainstem, basal ganglia, and cerebellum, but
χ ENCEPHALITIS LETHARGICA DEATHS
c By Month of Onset of Illness
O
∑
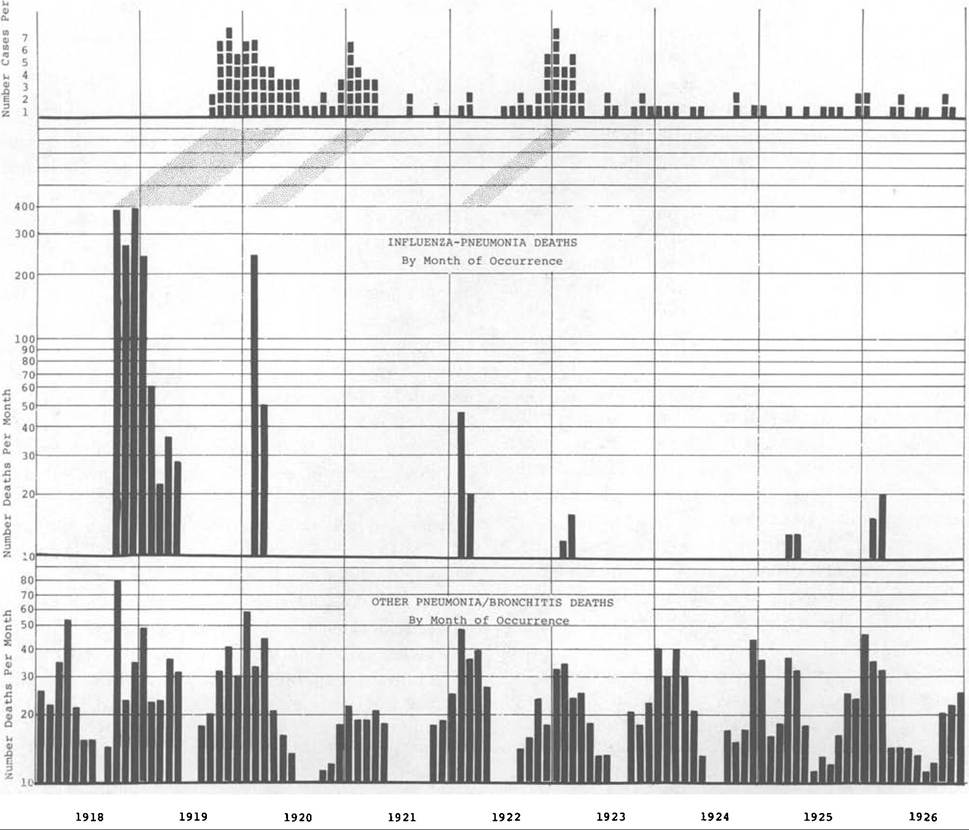
Figure VIIL46.1. Encephalitis lethargica, influenzapneumonia, other pneumonia/bronchitis deaths in Seattle-King County, Washington, 1918-26. (From
Ravenholt and Foege. 1981. 1918 influenza, encephalitis lethargica, parkinsonism. Lancet 2: 860-4, by permission of The Lancet.)
also including the cortex and the subcortical white matter. In the spinal cord, both the white and gray matter were involved in the inflammatory, degenerative disease process.
Epidemiology
The dominant epidemiological feature of encephalitis Iethargica was its unique time distribution. Although epidemics of encephalitic disease had occurred in conjunction with many previous influenza epidemics - 1580,1658,1673-5,1711-2,1729,1767, 1780-2, 1830-3, 1847-8, and especially 1889-92 - the global pandemic of encephalitis accompanying and following the 1918 influenza pandemic was in a class by itself with respect to virulence and sequelae. Along with its unique time distribution, 1917—26, the encephalitis Iethargica epidemic, as Figure VIIL46.1 indicates, also had a pronounced seasonal predilection for the winter months. Encephalitis cases often occurred in such close conjunction with individual and community attacks of influenza that many professional and laypersons initially believed the disease to be caused by the devastatingly virulent influenza. But the fact that many cases and epidemics of encephalitis subsequently occurred at times when, and in places where, there was no discernible influenza activity generated confusion and skepticism that influenza could be the principal cause.
Long latent intervals and slow viruses were not well recognized in 1918; hence encephalitis epidemics occurring a year and more after attacks of influenza were perceived as evidence against rather than supportive of influenza as the cause. Likewise, the fact that influenza was highly contagious and encephalitis was not was misinterpreted as indicating that these were unrelated diseases rather than being different manifestations of the same viral agent.Earliest reports of epidemic encephalitis in 1917 by Constantin Economo in Vienna and by French observers differed little in substance; but Economo’s provocative title, encephalitis Iethargica - giving unique emphasis to one sign in the broad spectrum of clinical manifestations - gained him lasting recognition while generating ongoing diagnostic confusion.
Although these reports of encephalitis preceded the explosive general global dissemination of influenza in 1918, influenza was active in war-torn Europe during the winter of 1916-17. In 1918, in close association with the initial massive waves of influenza, encephalitis was reported in Britain, Scandinavia, Germany, the United States, and many other countries; but the greatest epidemic peaks of encephalitis occurred in 1919-20 and during subsequent winters - as shown for Seattle in Figure VΠI.46.1.
Typically, encephalitis Iethargica was generally distributed by age, sex, race, occupation, education, economic status, and geographic location. Ages of cases ranged from infancy to old age, with the highest attack rates among young adults; and the sexes were equally represented. Rarely was there discernible clustering of encephalitic cases within families and neighborhoods; and where such was reported, it is retrospectively apparent that the clustering arose as a result of diagnostic confusion with other causes of central nervous system disease - for example, botulism.
Attack rates for encephalitis Iethargica during the pandemic years 1918-26 approached 1 case per 1,000 general population in the United States and in European countries where fairly complete records were maintained.
Of those afflicted, roughly one third died during their acute illness. Extensive but less precise reports from throughout the world indicate that attack rates for encephalitis Iethargica may have been similar worldwide, except in those few small populations, most notably American Samoa, where neither influenza nor encephalitis occurred during the pandemic years. Hence, the world total of encephalitis Iethargica cases was probably more than 1.5 million - of whom about 500,000 died of acute illness and more died from parkinsonism and other complications following the acute illness stage.Etiology
Despite the assertions of F. G. Crookshank (1919), RudolfvonJaksch (1923), and others that 1918 influenza was the principal cause of encephalitis lethargica, leading researchers of the 1920s, such as E. O. Jordan (1927) and A. J. Hall (1924), judged the relationship between influenza and encephalitis to be so inconsistent and confusing that they stated the etiology of encephalitis Iethargica to be “unknown.” But now, 60 and more years after the pandemic, from research done in Seattle and Samoa by R. T. Ravenholt and W. H. Foege (1982), the etiology of encephalitis Iethargica seems clear. Death records in Seattle show a characteristic modal lag of approximately a year from influenza-pneumonia death peaks to onset of encephalitis Iethargica clusters terminating in death (Figure VIII.46.1), providing strong evidence that encephalitis cases previously thought to have occurred independently of influenza were actually late sequelae.
The Samoan Islands were chosen as another site for study because the sharply contrasting experience of Western and American Samoa with respect to the 1918 influenza epidemic provided a unique basis for study of its pathological effects. As stated by Jordan:
In no part of the world did influenza exact a more crushing toll than in the islands of the South Sea. In Western Samoa the steamer Talune from Auckland introduced the disease on November 7,1918, into the islands of Upolu and Savaii.
As a result there were nearly 8,000 deaths, the population during the two months ended December 31, 1918, being reduced from 38,178 to 30,636.Meanwhile, American Samoa, just 70 kilometers away, and inhabited by the same racial stock, managed to exclude the infection with strict quarantine measures and good fortune.
During May 1982, American Samoa records stored in the National Archives and Records, in San Bruno, California, along with death records for American Samoa maintained by the Lyndon B. Johnson Tropical Medicine Center on Tutuila, and death records for Western Samoa available in the Registrar’s Office at Apia were analyzed. Although the rudimentary nature of the death records in Western Samoa limited the comparative studies that could be made of mortality patterns in American and Western Samoa during the 1920s, it was clear that whereas Western Samoa suffered heavily from both influenza-pneumonia and encephalitis Iethargica during the years 1918-22, American Samoa was remarkably free of both these diseases during those years. The evidence, then, is compelling that the pandemic of influenza beginning in 1918 and the pandemic of encephalitis Iethargica generally beginning the following year had a common etiology. Both pandemics were globally distributed and were closely related in time, and only one etiologic agent (swine influenza virus) has been reliably identified.
Local, regional, and national influenza-pneumonia epidemics ordinarily (perhaps invariably) preceded local, regional, and national epidemics of encephalitis lethargica. A large proportion of individual encephalitis Iethargica cases during the early years of the pandemic had had clinical influenza. Later, as influenza and encephalitis occurrence patterns shifted from massive epidemic to sporadic endemic, the relationship between these two diseases became progressively obscured.
Seasonal and global occurrence patterns of encephalitis Iethargica rule out the possibility that this pandemic was caused by an arbovirus or any known nonrespiratorily spread infection.
Moreover, although influenza-pneumonia was highly communicable from person to person, encephalitis Iethargica was remarkably noncommunicable from person to person by any known route.Analogous pandemics of encephalitis have been recorded in close association with other influenza epidemics, although none as severe as that in association with the 1918 influenza pandemic. Guillain- Barr6,s disease following inoculation with swine influenza antigen suggests a neurotoxic effect of this organism, even in the killed state. Likewise occurrence of parkinsonism during convalescence from influenza and/or encephalitis and during many years and decades thereafter demonstrates the extraordinary neuropathogenic qualities of the causative agent - now identified as the 1918 (swine) influenza virus.
Immunology
The immunologic findings of E. T Gamboa and colleagues in 1974 support the contention that the 1918 influenza (swine, type A) and encephalitis lethargica epidemics had a common etiology: They found deceased patients with well-documented postencephalitic parkinsonism to have intranuclear fluorescent antibody to neurotropic influenza A strain antigen in hypothalamic and midbrain sections, whereas no such fluorescence was observed in similar sections Table VIΠ.46.1. Time interval from encephalitis to parkinsonism to death in six patients
| Patient | Years from | ||
| Year of encephalitic illness | encephalitic illness to parkinsonism | Years from encephalitic illness to death | |
| 1 | 1925 | 1 | 47 |
| 2 | 1927 | 13 | 45 |
| 3 | 1924 | 2 | 48 |
| 4 | 1926 | 17 | 46 |
| 5 | 1921 | 12 | 51 |
| 6 | 1918 | 30 | 54 |
Source: Gamboa et al. (1974).
from brains of persons with idiopathic (not postencephalitic) parkinsonism. The long intervals between the several manifestations of 1918 (swine) influenza virus - pneumonia, encephalitis lethargica, parkinsonism - must be kept in mind when seeking to understand the interrelated epidemiology of these diseases (see Table VΠI.46.1).
History
From among all causes of encephalitis - structural, chemical, and microbiological - it was a difficult task sorting out the many infectious causes of encephalitis by specific causative organism and route of transmission. But with the explosion of scientific knowledge in the late nineteenth and twentieth centuries, many important agents and vectors of encephalitis were identified, among them, the spirochete of syphilis, and the trypanosome of African sleeping sickness, transmitted by sexual contact and tsetse flies, repectively; the bacterial toxin of botulism, from ingested food; the viruses of yellow fever, Japanese B encephalitis, equine encephalitis, transmitted by mosquitoes; the virus of rabies, transmitted by the bite of rabid animals; the viruses of influenza, mumps, and measles, transmitted by the respiratory route; the enteroviruses, transmitted by the fecal-oral route; and, most recently, the human immunodeficiency virus, transmitted by sexual contact and blood.
Adding to the diagnostic confusion generated by these numerous encephalitic microorganisms were the many cases and deaths from stuporous encephalitic reactions to various toxins and drugs, especially Reye’s syndrome following the use of aspirin (introduced in 1899) to control the fever and discomfort of influenza, varicella, and other childhood diseases. The role of aspirin in the production of Reye’s syndrome has become known only in the last decade.
But the main causative agent of epidemic encephalitis during the pandemic years 1917—26 was the respiratorily spread influenza virus. Successive peaks of encephalitis occurred in European, Asian, African, and American countries from 1918 to about 1926. In the United States, encephalitis Iethargica progressed across the country from the east to the west in 1919, just as influenza had the previous year, reaching peak occurrence in New York during January 1919, in Virginia during February, and in Illinois, Louisiana, and Texas during March; whereas in California more cases were reported in April than in any other month, and in Seattle the first encephalitis Iethargica cases were reported in October 1919. Although Britain reported its peak number of cases in 1924, this was apparently a reporting artifact - as judged from the mortality pattern during the 1920s.
For too long, medical science has tended to relegate the 1918 influenza-encephalitis Iethargica- parkinsonism puzzle to an intellectual ash heap, apparently on the assumption that these epidemics are past history and of little or at least dwindling importance to current and future health. But failure to identify influenza virus as the cause of encephalitis Iethargica and parkinsonism has crippled progress toward the understanding of influenza pathology and epidemiology needed to fuel and guide prevention of these elusive but exceedingly important diseases.
According to William Osler, Karl Menninger, and August Wimmer, almost every disease of the central nervous system (CNS) may follow influenza. Thus we should look to the diminutions of CNS structures caused by influenza attacks during earlier life when seeking the keys to prevention of much serious CNS disease, especially senile dementia (Alzheimer’s disease).
R. T. Ravenholt
Bibliography
Collins, S. D., and J. Lehmann. 1953. Excess deaths from important chronic diseases during epidemic periods, 1918-51. Public Health Monographs. U.S.P.H.S. Publication No. 213.
Crosby, A. W. 1976. Epidemic and peace: 1918. Westport, Conn.
Crookshank, F. G. 1919. Epidemic encephalomyelitis and influenza. Lancet 1: 79—80.
Economo, C. 1931. Encephalitis lethargica: Its sequelae and treatment, trans. K. O. Newman. London.
Gamboa, E. T., et al. 1974. Influenza virus antigen in postencephalitic parkinsonism brain. Archives of Neurology 31: 228—32.
Hall, A. J. 1924. Epidemic encephalitis (encephalitis lethargica). New York.
Jaksch, Rudolf von. 1923. Influenza encephalitis. Acta Medica Scandinavica 58: 557-84.
Jordan, E. O. 1927. Epidemic influenza: A survey. Chicago. Matheson Commission Reports I, II, III. 1929, 1932, 1939.
Epidemic encephalitis: Etiology, epidemiology, and treatment. New York.
Menninger, K. A. 1926. Influenza and schizophrenia: An analysis of post-influenzal “dementia praecox” as of 1918, and five years later: Further studies of the psychiatric aspects of influenza. American Journal of Psychiatry 5: 469-529.
Merritt, H. H. 1967. A textbook of neurology, 4th edition. Philadelphia.
Ministry of Health. 1924. Memorandum on encephalitis lethargica. HMSO, London.
Ravenholt, R. T., and W. H. Foege. 1982. 1918 influenza, encephalitis lethargica, parkinsonism. Lancet 2: 8604.
Shope, R. E. 1931. Swine influenza I: Experimental transmission and pathology. Journal OfExperimental Biology 54: 373-85.
Wimmer, A. 1924. Chronic epidemic encephalitis. London.
Winternitz, M. D., L. M. Wasson, and F. P. McNamara. 1920. The pathology of influenza. New Haven.