Epidemiology
When the science of epidemiology of the nineteenth century was applied to the study of yellow fever, the epidemiologist was hampered by a lack of knowledge of infectious agents and of vector arthropods in the transmission cycle.
Consequently, there was great confusion and an endless diatribe surrounding various hypotheses on how infection could travel so mysteriously from place to place, with infections occurring in people who apparently never had had contact with a case. With Theobald Smith’s demonstration in cattle of transmission of the Texas redwater fever organism by ticks, Ronald Ross’s demonstration of transmission of the parasite of malaria by mosquitoes, and Walter Reed’s demonstration of transmission of the virus of yellow fever by mosquitoes, came the dawn of modem epidemiological studies on arthropod-transmitted diseases.As can be seen in Table VIIL 10.3, a mysterious specificity exists between certain feeding arthropods and certain viruses; furthermore, a preferential feeding of certain arthropods (mosquitoes, for example) on certain food sources is shown. Some vertebrates react to a specific virus with severe disease. Yellow fever, for example, produces severe illness in humans, laboratory white mice, rhesus monkeys, and Alouatta monkeys. On the other hand, yellow fever
Table VIIL 10.2. Size, morphology, structure, and composition of selected virus families or generathat contain arboviruses
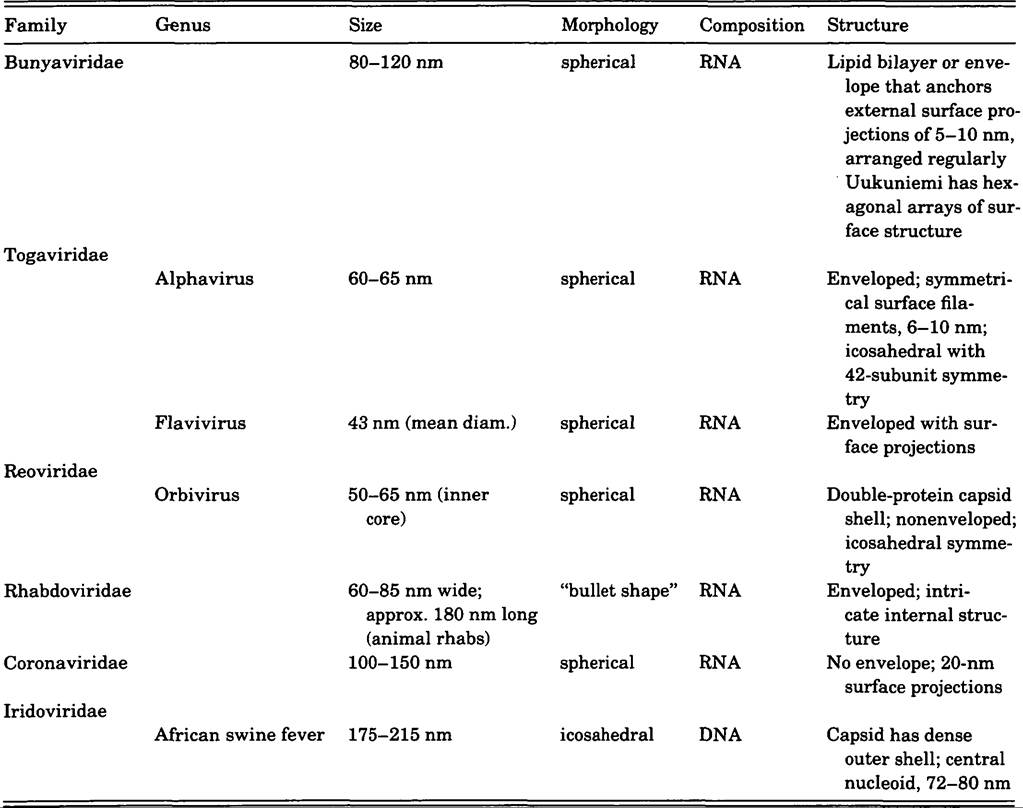
Source: In part based on Theiler and Downs (1973); Field (1985); and Monath (1988).
may infect dogs, cats, Cebus monkeys, cows, and horses without producing overt disease. Among the encephalitides, eastern equine encephalitis (EEE) virus (endemic strains) can produce severe disease and death in human beings, laboratory mice, certain other vertebrates, and very specifically equines.
But cattle do not develop illness with this agent, nor do sheep, goats, dogs, or cats. By contrast, the South American EEE strain that kills horses produces no illness in human beings but does produce detectable antibodies.The resistance of various vertebrates to various arboviruses can be of use to the investigator because it permits the production of large quantities of immune sera in such vertebrates. Such immune sera are of minimal importance in treating disease in human beings, but are of cardinal importance in the design of specific serologic tests for virus identification. With the advent of cell culture techniques, leading to the preparation of monoclonal antibodies to specific portions of a virus genome, identification work has been greatly broadened in scope and much narrowed in specificity, often providing in a matter of hours identification of a virus that would have required days or weeks for identification using older techniques.
Modem techniques, founded on studies carried out over a period of half a century, involving basic laboratory techniques of complement fixation, precipitation, electrophoresis, centrifugation, hemagluti- nation inhibition, and virus neutralization, have been extended by later advances such as “tagged”
Table VIIL 10.3. Twenty-nine selected arboviruses important in causing human andJor animal diseases, with data on vectors, hosts, and geographic distributions
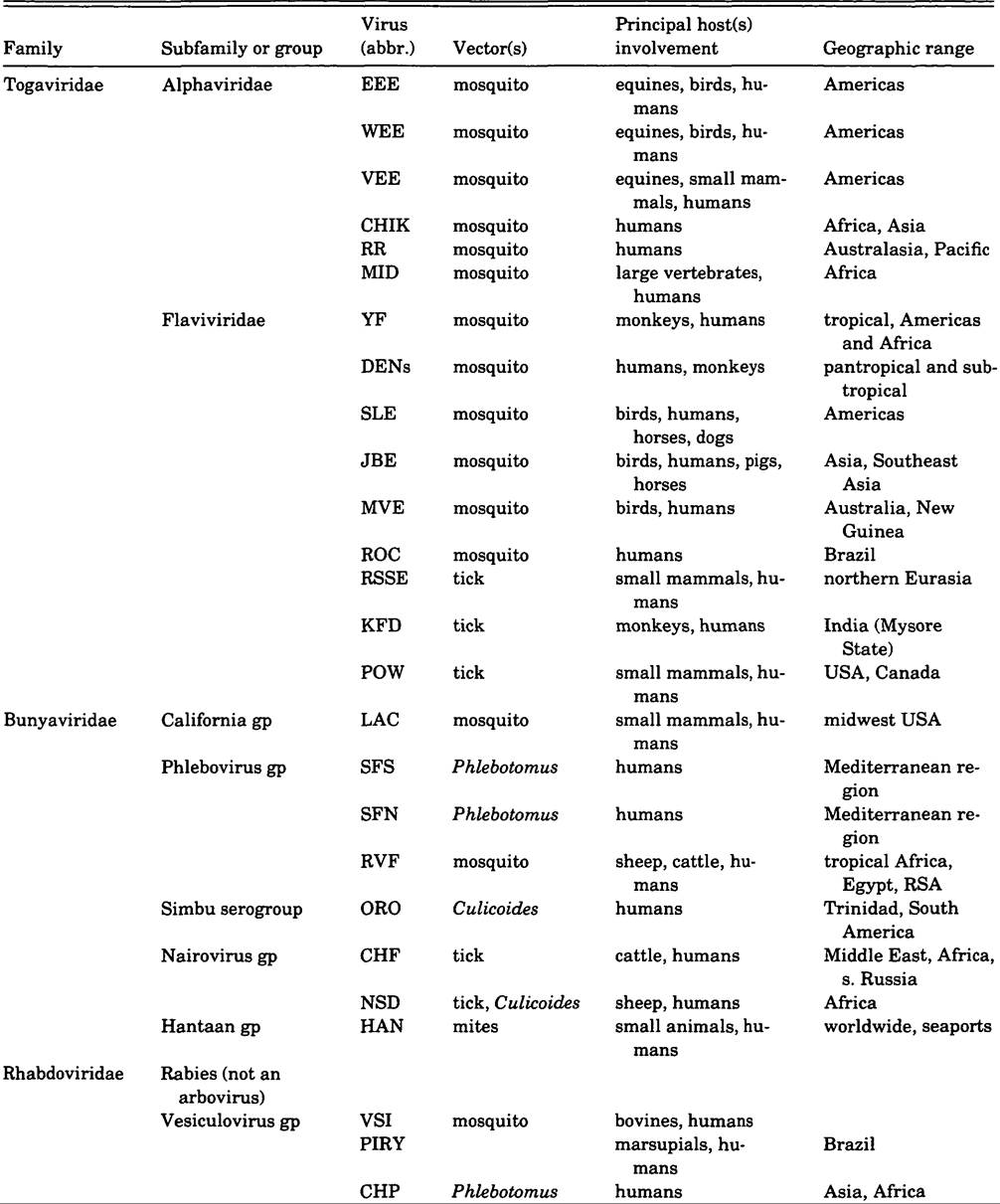
Table VIII.10.3. (cont.)
| Family | Subfamily or group | Virus (abbr.) | Vector (s) | Principal host(s) involvement | Geographic range |
| Orbiviridae | Colorado tick fever gp | CTF | tick | small mammals, humans | western USA |
| Changuinola gp | CHAN | Phlebotomus | humans | Panama, South America | |
| Iridoviridae | African swine fever | ASF | tick | swine, warthog | Africa, Europe, Cuba |
Abbreviations: ASF = African swine fever; CHP = Chandipura; CGL = Changuinola; CHIK = Chikungunya; CTF = Colorado tick fever; CHF = Crimean hemorrhagic fever; DENs = dengues (1,2,3,4); EEE = eastern equine encephalitis; HAN = Hantaan (Korean hemorrhagic fever); JBE = Japanese encephalitis; KFD = Kyasanur Forest disease; LAC = LaCrosse; MID = Middelburg; MVE = Murray Valley encephalitis; NSD = Nairobi sheep disease; ORO = Oropouche; PIRY = Piry; POW = Powassan; RVF = Rift Valley fever; ROC = Rocio; RR = Ross River; RSSE = Russian spring/ summer encephalitis; SFN = Naples sandfly fever; SFS = Sicilian sandfly fever; SLE = St.
Louis encephalitis; VEE = Venezuelan equine encephalitis; VSI = Vesicular stomatitis (Indiana); WEE = Western equine encephalitis; YF = yellow fever.Sources: Based in part on Calisher and Thompson (1985); Evans (1984); and Karabatsos (1975), among others.
antibodies - that is, the use of monoclonal antibodies in combination with “tagged probes” in electron microscopy. Such new techniques, involving the use of specific “probes,” are presently a fertile area of research, from which is emerging a more rational and complete knowledge of the virus particle itself and its interactions with vertebrate and invertebrate hosts.
Dengue
Geographic distribution of viruses and disease is determined by the characteristics of the vectors, rather than by the characteristics of the viruses. Taking dengue viruses (Flauiuirus genus) as an example, the limits of their distribution are defined by the limits of the distribution of the principal vector, Aedes aegypti. This mosquito, originally found in Southeast Asia, spread worldwide, traveling wherever humans traveled and established itself in tropical and subtropical and often temperate regions, but not in Arctic and Antarctic polar extremes. The dengue viruses moved with the vectors and became established worldwide, particularly in tropical and subtropical regions. The viruses may have had, in their original territories of Southeast Asia, cycles involving A. aegypti and/or Aedes albopictus and subhuman forest primates, but as the virus left their original home, they adapted to a vector-human- vector cycle, allowing them to exist in endemic form wherever humans exist, and to appear in epidemic form at intervals.
The other Southeast Asian vector, A. albopictus, has of recent years established itself in other countries such as the United States, with as yet unknown potential for involvement in the life cycles of still other viruses such as yellow fever. There are also other aedine vectors of dengue in Polynesia. The dengues are placed in four serotypes, one or more of which are associated with often fatal manifestations of dengue hemorrhagic fever and dengue shock syndrome.
These are important causes of mortality in small children in countries of Southeast Asia, scattered cases being seen elsewhere. It is hypothesized that sequential infections in the same individual by different serotypes of dengue may lead to these serious complications.Yellow Fever
Yellow fever, a Flaviuirus serologically related to the dengues, is also capable of being transmitted from human to human by A. aegypti and can maintain itself endemically in a human population by such means. This mode of transmission occurred a century and more ago but has not been observed recently. The virus is found in Africa, south of the Sahara, and in the equatorial South American jungle regions. In both Africa and South America (here including Central America, and the West Indies), and even in the United States, Spain, France, Gibraltar, and England, periodic outbreaks of the disease, often explosive and devastating, have been observed since A. aegypti may establish itself in subtropical and even temperate locales. Although A. aegypti (and A. albopictus) is prevalent in Asia and Australia, yellow fever has never established itself in these regions. With vectors present, as well as millions of nonimmune humans, there is a continuing threat of its introduction.
A reason yellow fever has been able to maintain itself in tropical South America and Africa is that the virus can utilize a different set of vectors: the forest canopy-frequenting Haemagogus mosquitoes of the New World, as well as A. aegypti and Aedes africanus, Aedes simpsoni, Aedes taylori, Aedes furcifer, and other aedines in Africa, often with and often without A. aegypti. Using the endemic Haemagogus or Aedes species, the virus remains established as an endemic virosis in various subhuman primates of these regions. This maintenance cycle is referred to as “sylvan” or “jungle” yellow fever. The sylvan Haemago- gus or Aedes can and often does bite humans, and thus can transfer the virus out of the mosquitomonkey-mosquito cycle into a mosquito-human- mosquito cycle.
An infected forest worker in the early stage of illness (and circulating virus in high titer) can migrate to an urban setting infested with A. aegypti and establish the dreaded urban mosquitohuman-mosquito cycle. Recently, several large outbreaks of this type have occurred in Africa and in South America, some of them involving the deaths of thousands of people such as in the Nigeria epidemic in 1986.A completely effective attenuated yellow-fever vaccine (17D) has been available since 1935, but governments in regions where yellow fever is endemic have as yet failed to react adequately in getting the population at risk immunized. The blame for this rests not on technical failure (the vaccine itself), nor on difficulties in administration of same, but in the inability of governments to establish adequate bureaucratic- administrative procedures to protect the health of the people. Aedes control projects, often employed for disease control, again suffer from a bureaucratic inability to maintain effective programs at a high level of efficiency over periods of years.
Encephalitides
Another group of the arboviruses, the encephalitides (Venezuelan, eastern, western, St. Louis, Japanese, Murray Valley, Russian spring-summer encephalitis), present mechanisms quite different from the dengue or yellow fever models. The vectors in question — mosquitoes or ticks - are of themselves geographically delimited, and therefore, the specific viruses associated with specific vectors are geographically delimited, with little chance of spread beyond natural ecological barriers. The viruses themselves have a basic vertebrate cycle in birds or small mammals. Certain of the viruses, such as Venezuelan equine encephalitis, eastern equine encephalitis, and western equine encephalitis, can escape from the mosquite-small vertebrate-mosquito cycle and spread like wildfire in one or another of the larger vertebrates, causing widespread mortality, and humans may be thus involved.
These epidemics are sporadic and unpredictable. The endemic cycles are present continuously, but unobserved unless specifically sought for. Others of the viruses are associated particularly with birds and mosquitoes. These viruses include St. Louis encephalitis virus of the Americas, Japanese encephalitis virus of the Orient, Murray Valley encephalitis of Australia and New Guinea, Ilheus virus of South America and Trinidad, Rocio virus of southeast Brazil, and West Nile virus of Africa, the Middle East, and India. The viruses are often very prevalent in a region, in birds, with the disease usually being uncommon in human beings, but sometimes occurring in large epidemics. Heron rookeries and pig farms in the Orient have been shown to be Japanese encephalitis virusamplifying localities, providing opportunities for infection of large numbers of mosquito vectors and thus facilitating large-scale transmission of virus to human beings. Immunity rates in populations are often high (bespeaking inapparent infections), and encephalitis rates low.In the central United States, a recent arrival on the virus scene, La Crosse virus, a member of the California virus group, has established its position as the commonest arboviral cause of encephalitis. This endemic disease has some unusual features. It is transmitted by woodland aedine mosquitoes, and has as vertebrate hosts certain small mammals of the region. It has been further established that the virus can be transmitted transovarially (TOT) from mosquito to mosquito, vertically, through the egg, and laterally, from female to male or from male to female during copulation. This mechanism has been hypothesized to explain the long persistence of virus in a vector, serving to carry it over periods of inclement weather or drought. Similar TOT has been shown for dengue, Japanese encephalitis, and yellow fever.
Tick-bome encephalitis (Russian spring-summer encephalitis, RSSE) in the Eurasian continent and Powassan virus encephalitis in America are delimited by the range of specific tick vectors; these viruses are endemic in small mammals and present themselves in humans as sporadic cases, often not distinguished from encephalitis caused by other viruses or of unknown etiology except by special laboratory studies.
Epidemiology of arboviruses can be conceptualized as a huge, multidimensional matrix, involving many viruses on one axis, many vectors on another, many vertebrate hosts on another, and yet another axis for ecological, ethological, meteorological, cultural, and edaphic influences impinging on vectors and hosts.
Clinical Manifestations and Diagnosis
The early days of onset of most arboviral infections are usually accompanied by fevers, aching, and general malaise, and cannot be distinguished from early stages of other very common diseases such as influenza, malaria, measles, pneumonias, meningitis, other respiratory afflictions, and even Lassa fever and smallpox. As diseases progress in their course, specific later manifestations may provide aid in differential diagnosis. Such specific manifestations include rashes, eruptions, nausea and vomiting, diarrhea, cough, and encephalitis.
Sporadic cases in a population may be quite impossible to diagnose specifically. But as epidemics progress, specific features may appear and provide the clue to diagnosis. Malaria in the tropics and influenza in temperate regions and the tropics serve as “coverup” or “umbrella” diagnoses that often block out recognition of arbovirus illness.
Definitive diagnosis demands the assistance of experienced virologists working in adequate laboratory diagnostic facilities. There exist only a few dozen such facilities in the world, supported by the World Health Organization, governments, armed forces military establishments, and, in a few instances, private philanthropy. Such laboratories usually combine laboratory diagnostic methodology and facilities for carrying out field epidemiological studies.
Specific diagnosis can only rarely benefit the patient, but is of vital importance in alerting health departments of the presence of a potentially threatening epidemic. Appropriate control procedures directed at the vectors can then be applied on an emergency basis. In the special case of yellow fever, mass immunization of exposed populations can successfully halt an epidemic in its tracks. Such an immunization campaign is usually combined with emergency mosquito control.