60 Glomerulonephritis (Bright’s Disease)
Glomerulonephritis, an immunologic disease of the kidneys, affects the glomerulus. This structure, a cluster of capillaries, is the filter in the functioning unit of the kidney, the nephron.
Inflammation, initiated by immune complexes (defined below), injures the glomerulus. Often the disease is acute, but it may be silent and completely undetected until signs and symptoms of chronic kidney failure prompt a biopsy, leading to diagnosis. Alternatively, this silent disease may prove fatal, and the diagnosis is made at autopsy.The urine-secreting structure (nephron) (Figure VIII.60.1) consists of the glomerulus and its tubular system. Each glomerulus consists of a tangle of interconnecting capillaries branching between two tiny arteries (arterioles). A glomerular cross section shows these capillary loops (Figure VIII.60.2). The glomerulus is a blood filter that controls passage of molecules through the basement membrane, depend-
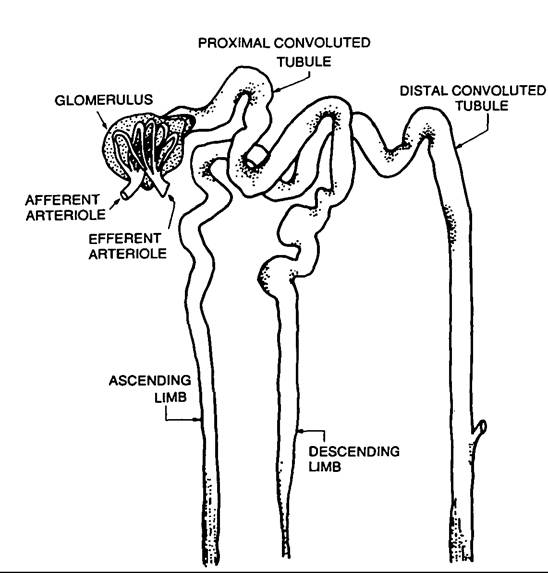
Figure VIII.60.1. Urine-secreting structure (nephron). (Modified from Arthur C. Allen. 1962. The Kidney: Medical and Surgical Diseases, 2d edition, 27, plate 13A. New York.)
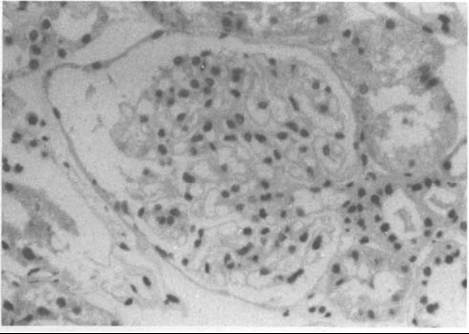
Figure VIII.60.2. Normal glomerulus. It consists largely of a tangle of tiny blood vessels (capillaries), many of which have been cut in a cross-sectional plane. They appear as spherical or oval empty spaces surrounded by a thin membrane. Many contain a nucleus (dark-stained spots) of the capillary lining (endothelial) cells.
ing on their size and charge. Normally red blood cells and albumin are not permitted to pass through the membrane. The tubules reabsorb, secrete, synthesize, and excrete solutes and metabolites, thereby maintaining physiological equilibrium.
This article will deal only with poststreptococcal glomerulonephritis. This disease, described by Richard Bright in the early part of the nineteenth century, still bears his name. Other forms of glomerulonephritis, which he also described, and the glomerular diseases termed glomerulopathies, seen in diabetes or amyloidosis, are not discussed.
Distribution and Incidence
Glomerulonephritis occurs worldwide. The disease was seen frequently in Europe during the eighteenth and nineteenth centuries as a complication of scarlet fever during epidemics. Today glomerulonephritis occurs sporadically. Several epidemics have occurred since the 1950s in the United States, Trinidad, and Venezuela. The disease would seem to be more prevalent in the Western world, probably only because modern diagnostic aids are available. Children contract it more commonly than adults, but it occurs in all age groups. Because the disease is often silent, the exact incidence of glomerulonephritis remains unknown.
Epidemiology, Etiology, and Immunology
For more than 200 years, physicians have known that swelling of the face and extremities (dropsy) occurred in some individuals IO to 14 days after bouts of scarlet fever (scarlatina). Early physicians believed that toxins, released during the fever, caused the dropsy, and long after Bright discovered the association of postscarlatina dropsy with changes in the kidney, the role played by scarlet fever still remained a mystery. These earlier beliefs were afforded credibility with the discovery, in the latter part of the nineteenth century, that the scarlatina rash resulted from streptococcal toxins.
It was only in the latter half of the twentieth century that F. G. Germuth (1953) and F. J. Dixon and others (1961) found that rabbits developed glomerulonephritis when given injections of a foreign protein (bovine albumin). About 2 weeks after these injections, the glomerulus sustained injury from immune complexes. An immune complex consists of an antigen (the protein), an antibody (produced by the rabbit), and a complement (humoral component).
Immune complexes localize in the glomerulus and damage the basement membrane. The damaged membrane leaks protein and red blood cells into the urine; swollen cells lining the capillary block the glomerular capillaries.In humans, events mimicking this model follow certain streptococcal infections caused by “nephritogenic” strains. Before the advent of antibiotics, glomerulonephritis usually followed an attack of scarlet fever. Today, in the Western world it more often follows streptococcal infections of the throat and skin, since scarlet fever is quite uncommon. Some part (still not identified) of the streptococcus serves as the stimulus for antibody formation.
Clinical Manifestations and Pathology
Signs of kidney disease usually follow infection, but not all patients have such a history. Many have no known or recognized antecedent illness. Generalized edema is often an early symptom. Red-brown or frankly bloody urine, reduced urine volume, hypertension, and headache from fluid accumulation are other common symptoms.
In children, poststreptococcal glomerulonephritis is usually a mild disease, and most children recover without permanent kidney damage. In adults, in contrast, permanent kidney damage occurs more often. The reasons for this difference are unknown.
The main pathological changes in glomerulonephritis are an increase in glomerular Cellularity (Figure VΠL60.3) and red blood cells in the tubules. With special studies, one can detect immune complexes in the glomeruli on the basement membranes. In an occasional individual, masses of cells, called epithe-

Figure VIII.60.3. Acute glomerulonephritis. As compared with Figure VIII.60.2, the glomerulus is larger and the nuclei (dark-stained spots) are both more numerous and swollen to the point of obliterating the capillary lumens, rendering them indistinguishable.
Iial crescents, surround the glomeruli, and strangle blood flow to the capillaries, causing kidney failure and death to the patient unless hemodialysis is undertaken.
History and Geography
Early Accounts Through the Eighteenth Century
Dropsy, a clinical finding, occurs not only in glomerulonephritis, but also in a number of other conditions and diseases including heart failure and end-stage liver disease. There are early accounts of dropsy, and some of these certainly refer to glomerulonephritis. Glomerulonephritis also causes bloody urine, but other common causes of this symptom include urinary tract stones, tumors, and parasitic diseases.
In the writings of Rufus of Ephesus, of about A.D. 100, we read of “hardening of the kidneys.” This was noted in patients who had only small amounts of urine, were free of pain, and who sometimes developed dropsy. This description could certainly be chronic glomerulonephritis. Ancient Hindu writings refer to dropsy attributed to heart disease. Avicenna, an Arabian physician and author of the Canon, perhaps the most famous medical text ever written, referred to patients with “chronic nephritis” around A.D.1000.
The treatise on surgery written by Gulielmus de Saliceto of Bologna about the middle of the thirteenth century but not published until 1476, has a reference to dropsy, scanty urine, and hardened kidneys. This is chronic kidney disease, and was very likely glomerulonephritis.
In another surgical text, Peter Lowe, a Scottish physician, wrote that “hydropsie” is a “Tumor against nature, engendered of great quantitie of Water, Winde, or Flegme, which sometimes is dispersed through the whole bodie, and is called Universali,” and “The cause interne of hydropsie... cometh... through the vice of the... kidneyes.”
Scientific urinalysis, representing a major step forward from the “looking and tasting” era of the Pisse Prophets, commenced with Frederick Dekkers, who discovered in 1695 that some urine samples, like serum, would coagulate with the application of heat or the addition of acetic acid. Today we know such a coagulum as albumin.
In the next century, Domenico Cotugno, an anatomy professor at Naples University, was attending a young soldier with a febrile illness, who “on the fifth day had a wonderful eruption of intercutaneous water.” This fluid and the urine each “contained a coagulable matter...
over the fire.” There is no indication that he knew of Dekkers’ observation, and Cotugno may be the first to have noted albumin in the urine, associated with dropsy.About this same time, Nils Rosen von Rosenstein, a Swedish physician, wrote an account of observations made during the scarlatina epidemic in Upsala in 1741:
But others... between the eighteenth and twenty second days, when the disease was to supposed to be quite cured... complained of weakness... and then the body began to swell, as in a dropsy [anasarca]; and upon this came on a fever, anxiety, uneasiness, oppression and asthma. Very little was discharged, and it is said to have been bloody in some patients, or appeared as water in which fresh meat has been washed.
This is an early, accurate account of poststreptococcal glomerulonephritis.
Nineteenth-Century Writings
The relationship between scarlet fever and dropsy was well recognized over the next 50 years. Thomas Bateman described eight patients with post-scarlatina dropsy seen between 1804 and 1816 in the public dispensary in London. At St. Thomas Hospital, William Charles Wells observed in 1811 that the urine in patients with dropsy after scarlet fever “contains almost always the serous, and sometimes the red matter of blood.” Unaware of Cotugno’s writings, he credits another with first noting, in 1798, “serum” in the urine of patients with dropsy. He looked for serum in the urine of 130 persons who had dropsy and found it present in 78 of the samples. He also noted that “urine in dropsy, when it contains serum, is often more abundant than in health.” (The increased urine volumes probably compensate for the loss of urine concentration in patients with failing kidneys.) He observed altered kidneys in one dropsical patient at autopsy who had serum in his urine, but with this limited observation did not feel justified in associating the findings with the kidney abnormalities, and wrote that “the morbid appearances in the kidneys might be altogether unconnected with morbid secretion....”
In 1818 John Blackall also observed dropsy, albuminuria, and bloody urine in patients after scarlatina.
Sometimes these patients at autopsy had “kidneys firmer than the ordinary, in one of them very strikingly so, approaching the scirrhus; but whether this is merely accidental, or the effect of such a course and what relation it bears to the discharge of serum must be left for future observations.”Those observations were soon to be made by Bright, a giant of medicine, who was conducting his landmark studies as a staff physician at Guy’s Hospital in London, on patients with post-scarlatina dropsy and albuminuria. In 1827, he first reported his findings and wrote, “The observations which I have made respecting the condition of the urine in dropsy, are in a great degree in accordance with what had been laid down by Dr. Blackall in his most valuable treatise.” Bright’s meticulously recorded accounts of the clinical features of the disease, and his colored illustrations of the pathological changes in the kidneys, remain a model for us today. He firmly established that dropsy was accompanied by pathological changes in the kidneys. His studies, however, did not address the question of how albumin enters the urine. This question could not be answered until nephron structure was further defined.
Marcello Malpighi had tried to answer the question in 1666 at Bologna. He knew of the glomeruli, and that they could be filled by injected dye into the blood vessels, but his frustration in being unable to establish their function is indicated in his writing:
I worked a long time in order that I might subject to the eye this evident connection [between “glands” and tubules] which reason sufficiently attests. For I have never been able to observe liquids perfused through the arteries penetrating the urinary vessels, even though they fill the glands, and the same is true when the veins are filled.... So that, in spite of many attempts (but in vain) I could not demonstrate the connection of the glands and the urinary vessels. (Italics mine)
In the early nineteenth century, the Berlin school, led by Johannes Peter Mueller, dominated anatomy and physiology in Europe. Mueller knew of Malpighi’s descriptions of the glomeruli, but he considered them to be simply receptacles of blood. He believed that urine was secreted by the epithelium of the proximal tubules.
But William Bowman in 1842 (then just 26 years old) wondered, as Malpighi had, why the glomerulus would end blindly in a space opening into the tubules. He wrote:
It would indeed be difficult to conceive a disposition of parts more calculated to favour the escape of water from the blood than that of the Malpighian body.... Why is so wonderful an apparatus placed at the extremity of each uriniferous tube, if not to furnish water, to aid in the separation and solution of the urinous products from the epithelium of the tube? This abundance of water is apparently intended to serve chiefly as a menstruum for the proximate principles and salts which this secretion contains, and which, in speaking generally, are far less soluble than those of any other animal product.
Bowman suggested that protein and red cells might pass through the glomerulus under abnormal circumstances!
A German physiologist, Carl Ludwig, followed up on Bowman’s anatomic Observationsjust a few years later, with the view that the glomerulus was a semi- permeable filter. Hydrostatic pressure pushed fluids through the capillaries that held back the proteins. In 1861 Thomas Graham showed that membranes could hold back colloids but permit the passage of crystalloids. The glomerulus was established as the source of urine, but albuminuria was still thought to come from tubular epithelium. For many years the term nephrosis was used to express this belief and define proteinuric states.
Through the rest of the nineteenth century, pathologists adhered to this view, even as microscopic studies advanced. The source of urinary albumin in dropsy was not determined for more than a century.
Bright’s descriptions of the kidney contained no records of microscopic examination. Rudolph Virchow established the cellular basis for pathology in 1858, and classified Bright’s disease into three categories - involving the tubules, the connective tissue, and the blood vessels. In some of his later writings, he referred to glomerular changes, but he continued to believe the main changes were in the tubules. The first pathologist to use the word “glomerulonephritis” was Edwin Klebs in 1879. The term became synonymous with Bright’s disease after F. Volhard and T. Fahr (1914, in Heptinstall 1983, Vol. 1) introduced it into their classification. That classification remained in use with little modification for nearly a half century.
The active use of biopsy to evaluate the nature of the kidney disorder in the patient was also an important clinical contribution. As biopsy experiences accumulated in the 1950s, 1960s, and 1970s, clinical and pathological classifications of Bright’s disease appeared in large numbers. Basic science investigators gave us an understanding of the important role of the immune system in glomerulonephritis, and they established the glomerular basement membrane as the site of leakage in albuminuric states. The tubule is not the source of the urine protein, but altered tubular reabsorption possibly plays a lesser role in albuminuria. The major contributions of pathology in the twentieth century are the use of thin sections, immunofluorescent techniques, and electron microscopy in biopsy interpretation.
Thus, today Bright’s disease consists of many different disorders, all of which can be considered glomerulonephritis. The diagnosis and management of these disorders will continue to challenge clinicians, pathologists, and basic science investigators into the twenty-first century.
Donald M. Larson
Bibliography
Bright, Richard. 1827. Reports of medical cases, selected with a view of illustrating the symptoms of cure of diseases by a reference to morbid anatomy. London.
1836. Cases and observations illustrative of renal disease accompanied with the secretion of albuminous urine. Guy’s Hospital Reports I: 338—400.
Castiglioni, Arturo. 1975. A history of medicine, trans. E. B. Krumbhaar. New York.
Dixon, F. J., J. D. Feldman, and J. J. Vazquez. 1961. Experimental glomerulonephritis: The pathogenesis of a laboratory model resembling the spectrum of human glomerulonephritis. Journal of Experimental Medicine 113: 899-920.
Germuth, F. G., Jr. 1953. A comparative histologic and immunologic study in rabbits of induced hypersensitivity of the serum sickness type. Journal of Experimental Medicine 97: 257-82.
Heptinstall1 Robert H. 1983. Pathology of the kidney, 2 vols. Boston and Toronto.
Major, Ralph H. 1932. Classic descriptions of disease. Springfield, Ill.
1954. A history of medicine, Vols. I and II. Springfield, ∏l.
Talbott, John H. 1970. A biographical history of medicine. New York.