69 Hypertension
Arterial hypertension is a condition characterized by abnormally high systolic and/or diastolic blood pressure levels. Systolic and diastolic blood pressure levels are usually estimated indirectly by use of an inflatable rubber bladder to compress the artery in the upper arm.
The pressure exerted on the artery by the bladder is registered by a device called a manometer. The level of the blood pressure is a measure of the force exerted against the walls of the artery during each heart beat or pulse. The peak of the pressure wave occurs when the heart beats or contracts (systole) and is called the systolic pressure. The valley of the pressure wave occurs when the heart relaxes (diastole) and is termed the diastolic pressure. Blood pressure is recorded as systolic over diastolic.Although longitudinal research studies such as the one in Framingham, Massachusetts, and the life insurance industry have noted that even slight elevations of blood pressure are associated with increased risk of premature death, the World Health Organization has recommended that the following blood pressure levels be used to classify adults (blood pressure levels defining juvenile hypertension are under review):
Hypertensive: Greater than or equal to 160 millimeters of mercury (mmHg) systolic and/or greater than or equal to 95 mmHg diastolic.
Normotensive: Less than or equal to 140 mmHg systolic and less than or equal to 90 mmHg diastolic.
Borderline Hypertensive: Between hypertensive and normotensive.
The condition is also divided etiologically into two types: secondary and primary or essential hypertension. Secondary hypertension, resulting from some known cause (including diseases of the kidney or the adrenal glands), represents less than 10 percent of all the cases of the disease. Essential hypertension, occurring in over 90 percent of the cases, is defined as high blood pressure without evident cause.
Most of the discussion that follows deals with this latter, more prevalent type of the disease.Distribution and Incidence
In most societies the average blood pressure levels and the diseases associated with higher blood pressure increase as people get older. However, blood pressure does not increase with age in all populations. Indeed, the disease appears to be totally absent from societies described as “stone age.” In such societies, blood pressure does not rise with age, and hypertension is extremely rare. However, a 1988 World Health Organization literature survey on high blood pressure in less developed countries revealed that the prevalence of hypertension there is increasing.
A recent international survey, the INTERSALT study, highlights the wide geographic variability of hypertension throughout the world. INTERSALT, a 52-center, 32-country study, found that the prevalence Ofhypertension (hypertensives were defined as anyone having greater than 140 mmHg systolic or greater than 90 mmHg diastolic or of persons on antihypertensive medication) between the ages of 20 and 59 ranged from zero percent in the Yanomamo Indians of northern Brazil to over 33 percent in an African-American population in Jackson, Mississippi. There was a significant within-continent variability as well (see Table VIII.69.1). It is likely that this wide variability in the prevalence of hypertension is due to differences in both environmental and genetic factors.
Etiology and Epidemiology
Many have hypothesized that environmental factors are primarily responsible for the development of high blood pressure. Principal evidence for this view consists of reports that Unacculturated or “primitive” populations are virtually free of hypertension, but when members of these populations migrate to urban areas their blood pressures rise. There are conflicting interpretations of this phenomenon: Some postulate that the change in diet (especially salt intake) and/or the weight gain that often accompany the move to a modern area are the primary reasons for the development of high blood pressure in populations that were previously free from it.
Others suggest that an increase in the level of psy- Table VIΠ.69.1. Prevalence Ofhypertension in 20- to 59-year-olds, by region, in ascending order by prevalence: 52 populations, INTERSALT Study, 1988| Rank of 52 | Prevalence hypertension (%) | Site, country (race) | n |
| Africa | |||
| 4 | 05.0 | Kenya | 176 |
| 42 | 24.0 | Zimbabwe | 195 |
| Asia | |||
| 2 | 00.8 | Papua New Guinea | 162 |
| 6 | 08.1 | South Korea | 198 |
| 7 | 08.5 | Beijing, P.R. China | 200 |
| 8 | 10.0 | Ladakh, India | 200 |
| 9 | 10.0 | Toyama, Japan | 200 |
| 10 | 10.9 | Tochigi, Japan | 194 |
| 11 | 11.7 | Osaka, Japan | 197 |
| 17 | 13.5 | Nanning, P.R. | 200 |
| 18 | 13.6 | China New Delhi, India | 199 |
| 20 | 15.0 | Tianjin, P.R. China | 200 |
| 28 | 17.6 | Taiwan | 181 |
| Europe | |||
| 12 | 12.5 | Iceland | 200 |
| 14 | 13.0 | Naples, Italy | 200 |
| 15 | 13.1 | Heidelberg, F.R. | 196 |
| 19 | 15.0 | Germany Birmingham, U.K. | 200 |
| 21 | 15.5 | Soviet Union | 194 |
| 22 | 15.5 | Torrejon, Spain | 200 |
| 23 | 16.0 | Manresa, Spain | 200 |
| 24 | 16.2 | Gubbio, Italy | 199 |
| 25 | 16.6 | Bernried, F.R. | 197 |
| 26 | 17.0 | Germany Ghent, Belgium | 200 |
| 30 | 18.6 | Belfast, U.K. | 199 |
| 31 | 19.0 | Krakow, Poland | 200 |
| 33 | 19.7 | Charleroi, Belgium | 157 |
| 34 | 20.5 | Mirano, Italy | 200 |
| 36 | 20.7 | German Democratic | 198 |
| 37 | 21.0 | Republic South Wales, U.K. | 199 |
| 39 | 23.0 | Joensuu, Finland | 200 |
| 40 | 23.0 | Malta | 200 |
| 43 | 24.2 | The Netherlands | 199 |
| 45 | 24.6 | Bassiano, Italy | 199 |
| 46 | 25.0 | Warsaw, Poland | 200 |
| 47 | 26.0 | Turku, Finland | 200 |
| 49 | 26.6 | Denmark | 199 |
| 50 | 31.0 | Hungary | 200 |
| 51 | 32.0 | Portugal | 198 |
Table VIΠ.69.1 (cont.)
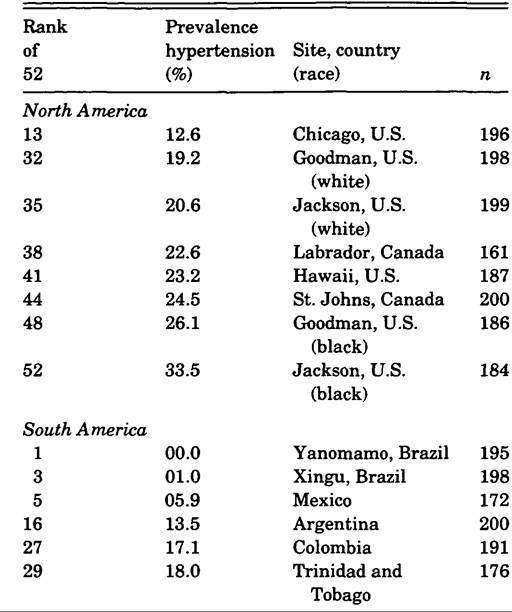
Note: At each site the investigators randomly chose about 200 individuals from population-based registries from 4 equally sized age groups between the ages of 20 and 59 years.
Subjects were defined as hypertensive if systolic blood pressure was ≥ 140 mmHg, or if diastolic BP was ≥ 90 mmHG, or if the subject was on antihypertensive medication. Total N = 10,079.Source: INTERSALT (1988).
chosocial stress is the culprit. Still others surmise that those who experienced the greatest rise in blood pressure may have inherited a genetic predisposition to the disease that is sparked by some environmental phenomena such as dietary salt or psychosocial stress. Interestingly, salt and stress have been assumed to be related to the disease for eons. A Chinese physician stated over 4,000 years ago that “if too much salt is used in food, the pulse hardens [and] when rebellious emotions rise to Heaven, the pulse expires and leaves the body.”
A gain in body weight as a result of a generalized increase in food intake is most definitely associated with high blood pressure, and a sustained reduction in body weight is one of the most effective methods of lowering blood pressure.
Specific dietary factors that may affect blood pressure include salt (sodium chloride), potassium, magnesium, calcium, fat, and even licorice. Most interest has centered around salt - more specifically, the sodium portion of the molecule. The most compelling evidence for the influence of salt on blood pressure is the fact that every low-salt-intake population ever studied has manifested very low blood pressure that does not rise with age. Significantly, INTERSALT reported a positive and statistically significant relationship between salt intake and blood pressure in their 52-center study.
Psychosocial stress is also believed to be associated with hypertension. In some population surveys, investigators have reported that societies under high stress also have higher mean blood pressure levels than those under low stress. Unfortunately, stress has been a difficult phenomenon to measure, and the association between stress and blood pressure has been difficult to demonstrate in human populations.
One of the most compelling animal models for stress- induced hypertension has been that developed by J. P. Henry and associates (1975). This model makes it necessary for mice to compete for food and territory; most animals in the system develop very high blood pressure and die from kidney failure. Notable exceptions are dominant males whose blood pressure is less elevated. Some believe that this is a valid model applicable to human societies as well.Heredity is known to be an important contributor to blood pressure regulation, and hence to abnormally elevated blood pressure or hypertension. Like many quantitative genetic traits such as height, levels of blood pressure tend to run in families; some have higher blood pressure, some have lower blood pressure. Other evidence of genetic influence is revealed by the concordance of hypertension in siblings, especially identical, or monozygotic (MZ), twins: If one member of a set of MZ twins has hypertension, there is a strong likelihood that the other will have the disease as well. Genetic influences on arterial pressure have also been demonstrated in inbred strains of rats, mice, and other animals. The hereditary mediators of these genetic influences on blood pressure are not known but probably reside in genetic influences on the major blood pressure control systems.
Many investigators believe that neither genetic nor environmental factors act alone, that in fact there is an interactive relationship between genes and environment. A compelling example of this is the simple breeding experiments in rats carried out by L. K. DahI and colleagues in the early 1960s. By selective breeding they were able, in a very few generations, to develop two strains of rats: One, extremely sensitive to the blood pressure-raising effects of salt in the diet, was called “salt sensitive”; the other, resistant to the blood pressure-raising effects of salt, was termed “salt resistant.” Humans manifest similar differences, in that some are “salt sensitive” and others are not, and the Dahl model may be applicable to understanding the evolution of “salt sensitivity” in human populations as well.
In former times, as isolated populations diverged and migrated into different ecological systems, they may also have experienced different “selection pressures” related to salt metabolism. These included different temperatures, salt intake, and mortality from salt-depletive diseases such as diarrhea and fever. These “selection pressures” may have resulted in a new genotype that enhanced survival in the new ecology environment by protecting against premature mortality from salt-depletive conditions. If this protective genotype included an enhanced ability to conserve sodium, then it is likely that these adaptations predispose to salt-sensitive hypertension today. It is argued that this may have occurred when many sub-Saharan Africans were forced to migrate to the Western Hemisphere. Mortality rates were very high from salt-depletive diseases, and it is surmised that those with the superior salt-retaining abilities survived and passed their genes on to present-day African Americans. This enhanced genetically based ability to conserve salt may, therefore, be found in greater frequency in Western Hemisphere blacks than in West African blacks, and may be part of the reason the former group today has a higher prevalence of hypertension than does the latter.
Clinical Manifestations
Although in the past a “hard pulse” or “dropsical swellings” (edema) may have signaled hypertension, today the only acceptable way to detect the condition is through the use of the blood pressure cuff (sphygmomanometer). Because the disease is usually asymptomatic, essential hypertension has been appropriately termed the “silent killer.” Undetected and uncontrolled, it can damage the arteries, the kidneys, and the heart, and, as several important long-term studies revealed, hypertension is a precursor to premature death from coronary heart disease, stroke, congestive heart failure, kidney (renal) failure, and atherosclerosis.
History
For centuries, the only way to assess “blood pressure” was to feel the pulse, and interpreting its force and rhythm proved to be a useful predictor of disease and death. In about 2500 B.C., for example, a Chinese physician remarked: “[W]hen the pulse is abundant but tense and hard like a cord, there are dropsical swellings.”
More than 4,000 years later, in 1827, the British physician Richard Bright suggested that the dropsical swellings he encountered in a patient were due to obstruction in the kidney’s circulatory system. Bright’s argument was so persuasive that throughout the remainder of the nineteenth century most physicians considered a strong or tense pulse a symptom of kidney disease.
By the late nineteenth century, the earlier discoveries on the measurement of systolic blood pressure by Stephen Hales, Samuel von Basch, and others led to the invention of the sphygmomanometer (blood pressure cuff). Coupled with the 1905 description of diastolic blood pressure by N. Korotkoff, this device effectively replaced diagnosis by “pulse,” and its widespread use led observers to the realization that most patients with elevated arterial pressure did not have a kidney disorder. This newly discovered condition was given various names including angiosclerosis, presclerosis, hyperpiesis, primary hypertensive cardiovascular disease, and essential hypertension. The condition was soon recognized as one of the most common types of cardiovascular disorders. Insurance companies led the way in quantifying the association between this new disease and premature death.
In the 1910s, the medical director of the Northwestern Mutual Life Insurance Company, J. W. Fisher, reported the results of several years of study of the relationship between blood pressure levels and premature death. Table VIII.69.2 provides a brief summary of the findings.
It was obvious to Fisher that the higher the systolic blood pressure, the greater the risk of death. Those with systolic blood pressure levels above 160 mmHg had a probability of premature death about 2.5 times greater than those with a systolic blood pressure of about 140 mmHg. In recommending that any insurance application with a persistent blood pressure of “15 mm Hg above the average for his or her age” should be investigated further, Fisher was probably the first to offer a quantifiable definition of “high blood pressure” (see Table VIII.69.3).
The scientific world was interested in what caused this newly discovered, deadly, and extremely prevalent disease. During the 1930s and 1940s, researchers conducted detailed examinations on the influence of the sympathetic nervous system, the endocrine system, and the renal system on arterial pressure, and were successful in cataloging several types of
Table VIΠ.69.2. Relationship between blood pressure and mortality: Northwestern Mutual Life Insurance Company, 1907-14
| Age | Insurance status | Systolic BP | Observed deaths | Expected deaths | Proportion obs/expected |
| 40-60 | insured | 142.43 | 85 | 91.17 | 0.93 |
| “All ages” | insured | 152.58 | 33 | 23.62 | 1.40 |
| “All ages” | not insured | 161.44 | 83 | 34.95 | 2.37 |
Note: Expected deaths = expected deaths in company (80% of M.A. table in source); systolic BP = systolic blood pressure; observed deaths = observed deaths of those with noted systolic blood pressure.
Source: Adapted from Fisher (1914).
secondary hypertension. Pheochromocytoma was first reported in 1929, Cushing’s syndrome in 1932, pyelonephritis in 1937, renal artery stenosis in 1938, and Conn’s syndrome (primary aldosteronism) in 1955. In very few cases these “secondary” causes of high blood pressure were cured through surgery, but in the great majority of cases - those with essential hypertension - the ultimate determinant of elevated arterial pressure remained a mystery. One very important breakthrough in understanding the pathophysiology of essential hypertension occurred among investigators working in animal physiology.
In the 1920s, Harry Goldblatt progressively constricted blood flow to the kidney in a dog, which produced a rapidly developing high blood pressure that resulted in death due to heart failure. The experiment, said by T. A. Stamey to have “stimulated more medical research than any single experiment in medical history,” sparked a worldwide search for a kidney (renal)-based pressor substance that produced hypertension. By the end of the 1930s, two
Table VIII.69.3. “Normal” and “unacceptable” systolic blood pressures by age: Northwestern Mutual Life Insurance Company, 1914
| Age group | “Normal” systolic blood pressure | “Unacceptable” systolic blood pressure |
| 15-20 | 119.85 | >134.85 |
| 21-25 | 122.76 | >137.76 |
| 26-30 | 123.65 | >138.65 |
| 31-35 | 123.74 | >138.74 |
| 36-40 | 126.96 | >141.96 |
| 41-45 | 128.56 | >143.56 |
| 46-50 | 130.57 | >145.57 |
| 51-55 | 132.13 | >147.13 |
| 56-60 | 134.78 | >149.78 |
Source: Adapted from Fisher (1914).
teams, one in the United States and one in Argentina, simultaneously discovered that the blood from a “Goldblatt kidney” contained a substance that caused vasoconstriction (squeezing of the arteries). The American group called their substance “angio- tonin,” while the Argentine group christened the compound “hypertensin.” These two teams met and, deciding they were working on the same substance, combined their two names for the compound; the substance became angiotensin. These discoveries led to extensive biochemical research into the neural, cellular, and hemodynamic systems that control blood pressure, and eventually to the development of the most widely prescribed antihypertensive medications today. The discovery and elucidation of the biochemical mechanisms controlling blood pressure were extremely important in understanding and controlling high blood pressure, but researchers were still a long way from finding the ultimate cause of the disease.
In the 1950s and 1960s, an important debate occurred between two British physicians over the influence of heredity on high blood pressure in humans. Robert Platt argued that essential hypertension was a “qualitative” disease, controlled by a single gene, with a bimodal population distribution. George Pickering, on the other hand, reasoned that what was termed “hypertension” was only the upper end of a continuous unimodal distribution of blood pressure levels. He thought that hypertension was a “quantitative” disease and was controlled by multiple genes in combination with environmental influences. The debate was never resolved by the two participants. Epidemiological research since then has tended to favor Pickering’s quantitative definition; however, in 1983 the analysis of a biostatistician showed the bimodal distribution of blood pressure values in a very large sample from Norway.
Today, both environmental and genetic factors are under intense study as possible etiologic factors at the individual level and the population level. However, it is still the case that the cause of abnormally elevated blood pressure in over 90 percent of the cases remains unknown. Fortunately, however, successful efforts are being made to lower blood pressure through diet, stress reduction, exercise, weight control, medication, and other means, in the hope that the frequency of premature deaths from hypertension will be reduced throughout the world.
Thomas W. Wilson and Clarence E. Grim
Bibliography
Allanby, K. D. 1958. The evolution of the treatment of essential hypertension. Guy’s Hospital Review 107: 515-30.
Dahl, L. K., M. Heine, and L. Tassinari. 1962. Role of genetic factors in susceptibility to experimental hypertension due to chronic excess salt ingestion. Nature 194: 480-2.
Fasciolo, J. C. 1977. Historical background on the reninangiotensin system. In Hypertension: Physiopathology and treatment, ed. E. Koiw Genest and O. Kuchel, 134-9. New York.
Fisher, J. W. 1914. The diagnostic value of the sphygmomanometer in examinations for life insurance. Journal of the American Medical Association 63: 1752-4.
Flexner, M. 1959. The historical background of medical therapy in essential hypertension. Journal of the Kentucky Medical Association 57: 1210—13.
Henry, J. P., P. M. Stephens, and G. A. Santisteban. 1975. A model of psychosocial hypertension showing reversibility and progression of cardiovascular complications. Circulation Research 36: 156—64.
INTERSALT Cooperative Research Group. 1988. INTERSALT: An international study of electrolyte excretion and blood pressure. Results from 24 hour urinary sodium and potassium excretion. British Medical Journal 297: 319-28.
Janeway, T. C. 1915. Important contributions to clinical medicine during the past thirty years from the study of human blood pressure. Bulletin of the Johns Hopkins Hospital 26: 341—50.
Kannel, W. B., M. J. Schwartz, and P. M. McNamara. 1969. Blood pressure and risk of coronary heart disease: The Framingham study. Diseases of the Chest 56: 43—52.
Kaplan, N. M. 1986. Clinical hypertension. Baltimore.
Laragh, J. H., and B. M. Brenner, eds. 1990. Hypertension: Pathophysiology, diagnosis, and management, 2 vols. New York.
Lew, E. A. 1973. High blood pressure, other risk factors and longevity: The insurance viewpoint. American Journal OfMedicine 55: 284.
Major, R. 1930. The history of taking blood pressure. Annals OfMedical History 2: 47—55.
Nissinen, A., et al. 1988. Hypertension in developing countries. WorldHealth Statistics Quarterly 41: 141-54.
Page, I. H. 1988. Hypertension research: A memoir, 19201960. New York.
Ruskin, A. 1956. Classics in arterial hypertension. Springfield, Ill.
Stamey, T. A. 1963. Renovascular hypertension. Baltimore.
Swales, J. D., ed. 1985. Platt versus Pickering: An episode in recent medical history. London.
Wakerlin, G. E. 1962. From Bright to light: The story of hypertension research. Circulation Research 11: 131— 6.
Waldron, I., et al. 1982. Cross-cultural variation in blood pressure: A quantitative analysis of the relationships of blood pressure to cultural characteristics, salt consumption, and body weight. Social Science Medicine 16:419-30.
White, P. D. 1946. The heart in hypertension since the days OfRichard Bright. Canadian Medical Journal 54: 129-36.
Wilson, T. W, and C. E. Grim. 1992. Unnatural selection: The history of the trans-Atlantic slave trade and blood pressures today. In The Atlantic slave trade: Effects on economics, societies, and peoples in Africa, the Americas, and Europe, ed. J. E. Inikori and S. Engerman, 339-59. Durham, N.C.
World Health Organization. 1988. Arterial hypertension. Technical Report Series N. 628.