II.6 Concepts of Cancer
In past centuries people feared epidemic diseases with their sudden onset, ghastly symptoms, agonizing death for many, and sometimes disfigurement or physical impairment for survivors.
Today, especially in the developed world (with a few notable exceptions), the dread of epidemic contagion seems almost as anachronistic as the burning of witches. It has been replaced by the dread of cancer. As with the epidemics of yesterday, the basic causes of cancer remain shrouded in mystery, while its effects in terms of human suffering are all too well known.Cancer is a process whereby a loss of control of normal cell division and multiplication produces a tumor that can invade adjacent tissues and metastasize, that is, implant cancerous cells at a site that is noncontiguous to their origin, where abnormal multiplication continues. When cancer originates in connective tissues (mainly bone or muscle), it is called sarcoma; when it originates in epithelial tissues (lining tissues and organs such as the breast, lungs, or stomach), it is called carcinoma. The latter is by far more common. Invasive tumors occur in all complex species and probably antedate the advent of vertebrates. The oldest paleopathological evidence is limited to lesions that affected bones, such as those found in dinosaurs. Tumors have been found in Egyptian mummies dating from 2000 to 3000 B.C., and physicians of that ancient land knew of and treated patients for cancers of several sites.
Certainly the ancient Greeks were familiar with this disease, or perhaps better, this group of diseases. The condition is discussed in the Hippocratic corpus, and in fact its nomenclature is dominated by Greek words. Hippocrates himself is credited with having named the disease cancer from karcinos, the Greek word for crab, perhaps because some cancers of the breast have a crablike appearance or perhaps because the pain that cancer can produce resembles the pinching of a crab.
Similarly, neoplasm, meaning “new formation,” and oncology, literally the “study of masses,” are derived from the Greek, as is the word tumor.Hippocratic medicine attributed tumors-which included all sorts of swellings - to an abnormal accretion of humors. Although some remedies are mentioned, aphorism VI.38 advocates conservatism: “It is better not to apply any treatment in cases of occult cancer; for, if treated, the patients die quickly; but if not treated they hold out for a long time.” Galen sought to differentiate more clearly cancers from inflammatory lesions and gangrene. Cancer was held to be caused by black bile; if the cancer ulcerated, the black bile was undiluted; if there was only a tumor, the pathogenic humor had been diluted.
Carcinoma of the breast was probably the earliest actual neoplasm for which surgical eradication was attempted. Leonides of Alexandria, who slightly preceded Galen, is known to have progressively incised and cauterized, both to prevent bleeding and to destroy the neoplasm. Galen, conversely, recommended that bleeding be permitted, presumably for the pathogenic humor to be drained. Some surgeons performed a total mastectomy. Little was written about the healing of these terrible procedures, but Rhazes warned in the ninth century that those who performed surgery on a cancer generally only caused it to worsen unless it was completely removed and the incision cauterized.
Although barber-surgeons probably incised and excised boils and warts in the belief that they were curing cancer, it seems likely that few cancers were treated surgically until relatively modem times. Ambroise Pare wrote toward the end of the sixteenth century that those who pretended to cure cancer Siwgically only transformed a nonulcerous cancer into an ulcerated one. “I have never seen a cancer cured by incision, nor known anyone who has.” Nevertheless, in the seventeenth century, Wilhelm Fabricius of Hilden described the removal of axillary nodes in a breast cancer operation and provided adequate descriptions of operations for other cancers.
The discovery of the lymphatic system by Gas- parro Aselli in 1622 directed medical attention away from the black bile theory, which no one had demonstrated, toward abnormalities of the lymphatic structures in the causation of cancer. Basically, the idea was that cancer was an inflammatory reaction to extravasated lymph, the type of lesion depending on its qualities. About 150 years later John Hunter modified the lymph theory by defining “coagulating lymph” (i.e., blood serum), as opposed to true lymph, as that component of blood that clotted spontaneously when it was extravasated. It was this “lymph,” when it was contaminated by a “cancerous poison” and oozed into tissues, that Hunter viewed as the cause of cancer. Quite presciently, he described metastases as “consequent cancers” that reached distant parts via lymphatic channels.
A more transitory hypothesis advocated particularly by the German Daniel Sennert and the Portuguese Zacutus Lusitanus early in the seventeenth century was that cancers, at least when ulcerated, were, like leprosy, contagious. Popular fear of the contagiousness of cancer persisted into the twentieth century. The first accurate etiologic observation about any cancer can be attributed to the London surgeon Percival Pott, who reported in 1775 that many men who had worked as chimney sweeps since boyhood and were routinely lowered into narrow chimneys suffered scrotal cancer. He linked this observation to the irritating effect of chronic contact with soot and thereby identified the first occupational cancer.
The impact of microscopy on cancer research came very slowly. Robert Hooke, the pioneering seventeenth-century microscopist who coined the term cell, thought that tissues were composed of fibers-a hypothesis that persisted into the nineteenth century. Not until after 1830, when Joseph J. Lister designed the first achromatic microscope lenses, did progress in histology begin, made mostly by German investigators. The first new concept, advanced by Theodor Schwann and supported by Johannes Mueller, was that all tissues were composed of microscopic cells, not fibrils.
Yet the lymphatic theory was not easily abandoned, and cells were thought to derive from “blastema,” which was organized from intercellular fluids. In 1854, however, Rudolph Virchow questioned the existence of the unidentified blastema, and in the following year he stated the principle that all cells originated from cells and postulated that neoplasms developed from immature cells. But even then the spread of cancer was considered to result from some sort of a humor rather than the dissemination of cells. In 1867 Edwin Klebs advanced the opinion that most cancers originated in epithelial tissues (carcinomas in modern terminology), and coincidentally, Wilhelm Waldeyer applied the old, previously unspecific term sarcoma to neoplasms that arose in connective tissues.Despite these scientific developments, cancer research is usually viewed as a twentieth-century Imdertaking and, despite its antiquity, the disease itself is viewed as largely a twentieth-century phenomenon. As infectious ailments have receded, cancer, along with cardiovascular diseases, has been perceived to be the greatest single health problem facing the developed world. Actually, cancer presents a set of problems, because the term should be considered a collective noun. The World Health Organization has classified some 100 kinds of cancer depending on their sites of origin, a figure that may be too conservative.
It is generally estimated that some form of cancer will develop in one-third of the inhabitants of the industrialized world. Moreover, the probability is increasing. Less than two decades ago it was calculated that one in four would develop cancer - with even those odds prompting the charge that cancer represents the “failure of medicine” (Braun 1977). Certainly this seems to be the case when a comparison is made with medicine’s triumphs against epidemic illnesses, which came one on top of the other after the advent of the germ theory. Although we are well into the second century since the beginnings of cell theory, cures for cancer have thus far largely eluded scientific medicine.
Nor has Virchow’s observation that irritants could summon forth cancerous cells proved very helpful in cancer prevention- although irritants are among the foci of cancer research today.The concept of autonomy suggests that once a cell has become truly cancerous it is beyond bodily control. The concept was established around the turn of the century by Arthur Hanau, Leo Loeb, and Carl O. Jensen, who transplanted cancer cells into healthy animals and plants of the same species and observed the unrestrained growth of new cancers in the previously healthy hosts. Yet the fact that cancers, once established, can enter a stage of remission - sometimes permanently - argues that the body can rally to retard or even reverse previously uncontrolled cell proliferation.
Following these transplantations, the next advances in research were made when cancer was produced experimentally in plants and animals by the administration of various chemical, physical, and biological agents. These experiments revealed, for example, that some 150 different viruses cause tumors in living organisms, that ultraviolet light and X-rays as well as radioactive substances such as radium and uranium induce cancer, and that coal tars, dyes derived from them, and other substances can also induce the disease. Moreover, even natu-
Table II.6.1. Ten most common invasive neoplasms and estimated new cases as percentage of all new cases in the United States, 1990
Neoplasm
Percentage Cases
Male
Prostate 21.1 30,000
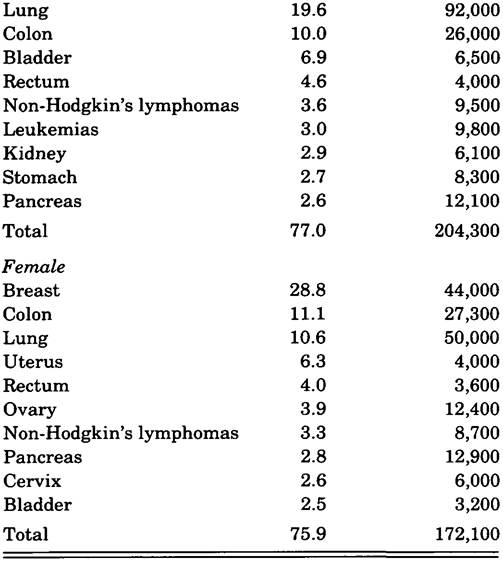
Table II.6.2. Deaths due to cancer as percentage of all deaths according to sex and age group, United States, 1986
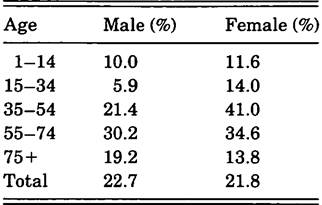
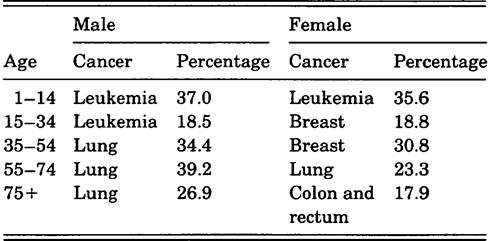
Table II.6.3. Most common cancers as causes of death from cancer, according to sex and age group, United States, 1986
rally occurring substances in the body, such as the sex hormone estrogen, have been shown to cause cancer when given to experimental animals.
The extent to which the incidence of cancer is increasing is a complicated issue. It is predominantly an illness of middle age and, with the exception of a few forms, such as certain leukemias, it is relatively rare in children. Thus, people in the developed world, having escaped famine and epidemic disease, have had their life expectancy extended beyond 50 years of age into that age in which the frequency of cancers becomes increasingly high. Although a shift in the age distribution of a population affects the actual incidence of cancer, the statistics have also shown artifactual increases. These are due to vast improvements in the diagnostic techniques of endoscopy, imaging, and biochemistry that can now be used to detect many asymptomatic cancers and pathological techniques that facilitate the differentiation of neoplastic from inflammatory lesions, primary from secondary neoplasms, and so forth.
The following interpretation of the most recent U.S. cancer statistics offers some quantification of the impact of the disease in relation to age, sex, and race (see Tables II.6.1 through II.6.4). The three most common cancers of men, those arising in the prostate, lung, and colon, comprise about 50 percent of new cases and 55 percent of deaths due to cancer. The three most frequently occurring cancers of women, breast, colon, and lung, also comprise about 50 percent of new cases and account for 50 percent of deaths. As a proportion of all deaths, those from cancer do not increase linearly with age. This is mainly because of the accidental deaths of children and young adults, on the one hand, and cardiovascular diseases in the elderly, on the other. Of deaths from cancer in women, the peak, 41.0 percent, occurs in the 35 to 54 age group. In contrast, men have a somewhat older average age of death with 30.2 percent in the 55 to 74 age group. Most of this difference is attributable to the difference in the age distribution of women with carcinoma of the breast and men with carcinoma of the prostate. Smwival has improved variably from the 1960s to the 1980s. The Table ∏.6.4. Five-year survival rates by race in two time periods from principal malignant neoplasms in the United States
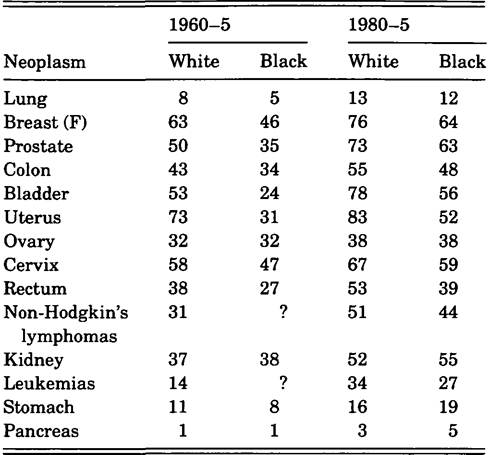
Note: Data are percentages.
Source: Data through 1986 from state records of Connecticut, Hawaii, Iowa, New Mexico, Utah, and Atlanta, Detroit, Seattle-Puget Sound, San Francisco-Oakland.
greatest improvements have occurred in the treatment of stomach cancer in both sexes and in uterine cancer. Of the more common neoplasms, only lung cancer has increased in incidence in both sexes, as has carcinoma of the prostate in men. Survival was below 20 percent for four of the more common neoplasms in the 1960s (leukemias, stomach, lung, pancreas), and save for the leukemias, it remains below 20 percent. The explanation for the decrease in death from stomach cancer lies in a decline in its occurrence, not by a great improvement in therapeutic success. Survival generally has been and remains poorer for black than for white patients. In 1960 white patients had a 42 percent better chance than their black counterparts of survival following treatment of carcinoma of the uterus, a 29 percent better chance with carcinoma of the bladder, and a 17 percent better chance with carcinoma of the breast. In 1980 the greatest race-related survival differences were such that whites had the following better chances than blacks: carcinoma of the bladder, 22 percent; carcinoma of the uterus, 21 percent; and carcinoma of the rectum, 14 percent. These differences have often been attributed to the black population’s poorer access to medical care. However, this is obscured by the fact that there do not seem to be race-related differences in survival of other relatively common carcinomas such as those of the lung, kidney, and stomach.
For the incidence of a disease to be considered meaningfully, it must be presented in age-specific terms. As the average age of a population increases and the proportion of an age group in which various cancers most commonly occur becomes larger, an increase in the number of cases is to be expected. This increase, however, can tend to blur the more important question of whether the incidence of that disease is increasing in a specific age group. The statistical analyst must also be cognizant of the impact of technological improvements on the finding of potential cases and the establishment of a diagnosis, as well as changes in interest in the disease in question and changes in access to medical care.
Moreover, the addition to or removal from the environment of a carcinogen is a convenient explanation for the waxing or waning of the occurrence of a cancer. In this regard the long latent period of most clinical cancers is often overlooked. For example, an argument used in the 1940s against the hypothesis that cigarette smoking was a major cause of lung cancer was that many more women were smoking than had previously been the case, yet no increase in lung cancer among women had occurred. Consequently, the relationship between smoking and Itmg cancer in men was viewed by some to be coincidental rather than causal. But of course, in retrospect we can see that most of the women in question had not yet smoked for a sufficient length of time for the result to become evident in cancer statistics. Perhaps future analysis will clarify in a similar fashion why gastric cancer is decreasing in the United States or why prostate cancer is increasing. Certainly one of the most difficult problems in identifying causes of cancer is that of cocarcinogenesis. The most flagrant example is the additive effect of the inhalation of both cigarette smoke and asbestos particles on the occurrence of lung cancer. Both of these agents are independently carcinogenic, and their combined effect greatly increases the incidence of the disease.
With regard to public health, the greatest problem of exogenous carcinogenesis today is not exposure to industrial pollutants, as many believe, but rather the use of tobacco products. Whereas cigarette smoke appears to exert the most potent carcinogenic effect, cigar smoke and chewing tobacco are also implicated. Historically, the possibility that an increase in lung cancer was related to an increase in cigarette smoking was first raised in Germany in the 1920s. In the United States interest in this question was stimulated in 1950 with the publication of three epidemiological studies, each of which showed that lung cancer patients were likely to be heavy smokers.
Although an epidemiological association cannot prove a causal relationship, the satisfaction of five criteria make such a connection highly probable: (1) The association between the suspected pathogen and the disease is observed consistently. (2) In comparison with suitable control groups, the association is strong. (3) The association is relatively specific with the disease in question. (4) The temporal relationship between exposure to the pathogen and the onset of the clinical disease is appropriate and consistent. (5) The association is consistent with a known or plausible explanation of the natural history of the disease.
Resistance to the acceptance of a causal relationship between smoking and the development of lung cancer was based initially on doubt that the incidence of lung cancer was actually increasing and then on a failure to appreciate the long preclinical phase of the disease. A massive prospective study of the effects of smoking on health published by E. C. Hammond and D. Hom in 1958 purported to show that smoking was not uniquely associated with lung cancer.
Similarly, the observation that cigarette smoking was associated with neoplasms of organs, such as the bladder, which did not come into contact with smoke, and with’cardiovascular diseases was used by proponents of tobacco interests and some biostatisticians to cast doubt on a causal relationship between the inhalation of cigarette smoke and the development of lung cancer. This argument ignored the multiplicity of components of tobacco smoke, which could easily act differently on different tissues, and the clearly quantitative relationship between smoking and the increased probability of lung cancer developing. Nevertheless, lung cancer occurs in a small minority of even heavy smokers. This has been taken to indicate an intrinsic predisposition that, if identified, could be used to warn persons at risk. But investigations have thus far failed to yield useful results. Finally, there have been no reproducible experiments in which tobacco smoke has caused lung cancer in experimental animals. Although positive results would be convincing, negative results are attributable to species differences and, perhaps, insufficient duration of exposure.
Eight prospective studies of male cigarette smokers have shown an excess mortality from lung cancer in comparison with nonsmokers ranging from 3.8 to 14.2 percent (mode 11 percent). In four studies of women the excess was smaller, ranging from 2.0 to 5.0 percent. Despite the fact that no specific sufficiently potent pulmonary carcinogens have as yet been identified in tobacco smoke, a 1970s finding appears to clinch the causal relationship between smoking and the development of lung cancer. R. Doll and R. Peto (1976), in a 20-year investigation of the mortality of British physicians in relation to smoking, showed that the risk diminishes increasingly after smoking has been discontinued for several years. This obviously cannot be ascribed to genetic or psychological factors. However, even 15 years after cessation the risk among former smokers remained twice that of men of similar age who had never smoked.
Smoking has now been common among women long enough to be reflected in an alarming increase in the incidence of lung cancer. This began in the mid-1960s, and the incidence now is half that of men in the United States. As of 1986 the rate of death from lung cancer for U.S. women equaled that for breast cancer, which has remained stable. In the case of the latter disease it appears that, of the halfmillion women worldwide in whom breast cancer develops annually, half reside in North America and western Europe, which contain less than 20 percent of the world’s population. However, it is hazardous to compare prevalence or even mortality statistics without knowing critical local circumstances. For example, why would the age-adjusted rate of death from breast cancer in Finland and Denmark be more than triple the rate in Sweden, and why would the rate in Scotland be quintuple that of England?
A daughter or sister of a woman with breast cancer has a nearly three times greater risk of developing this disease than a woman without such an association. The risk is greater if the relative’s cancer was found at an early age, and a great deal more if both mother and sister have been affected. This suggests a genetically mediated predisposition, as does the increased risk of a secondary primary breast cancer as compared with the risk of a first occurrence. However, other observations indicate that environmental factors must also enter in. For example, the prevalence of breast cancer in Japan is about one-fourth that in northern Europe or North America. Nevertheless, among women of Japanese ancestry living in North America, the incidence of breast cancer by the second generation matches that of white North American women. Whether dietary or other potential cofactors are implicated remains unresolved.
Unfortunately, cancer statistics often reveal the complexities of the disease under investigation rather than causal explanations. Carcinoma of the prostate is the second most frequently occurring cancer among U.S. men; it is the fifth worldwide. This disease is more prevalent among U.S. blacks, despite their heterogeneity, than any other population that has been studied. It is about 80 percent more common in black than in white men in the United States. It is also common in black Caribbean populations, whereas sketchy information from Africa indicates much lower prevalences. Carcinoma of the prostate is 28 times as common among blacks in Atlanta as among Japanese in Osaka. Although the incidence appears to be low throughout the Orient, it is much higher among men of Chinese and Japanese extraction living in Hawaii.
The incidence of clinically evident prostate cancer is more highly correlated with increasing age above 50 than is any other neoplasm. It is six to seven times more prevalent in the 75 to 84 than the 55 to 64 age group, and the black-white difference in prevalence diminishes with increasing age. There is no convincing evidence of the pathogenicity of any industrial exposure for this neoplasm. However, an increased risk is associated with chronic cigarette smoking, and there appears to be a correlation between an above-average sexual drive and susceptibility to prostatic carcinoma. This could mean that a subtle alteration in the metabolism of sexual hormones has a predisposing role, but studies have yielded inconsistent results. Alternatively, men with a high sexual drive, particularly in a permissive culture, have an increased likelihood of exposure to multiple sexual partners. A correlation between promiscuity and prostatic carcinoma, if substantiated, would suggest an analogy to the better-documented correlation between promiscuity and carcinoma of the cervix in women and the possibility that a sexually transmitted virus is a pathogenetic agent. None of these hypotheses, however, explains the increase in the occurrence of this disease in the late 1900s.
With regard to possible roles of diet in carcinogenesis there has been particular interest in whether the presence or deficiency of certain components of food influences the development of colorectal cancer. Both diets low in fiber and high in fat have been proposed to be pathogenetic. Investigations have yielded conflicting results, but the best evidence now points to a carcinogenic effect of increased fat consumption, particularly in women. Colorectal cancer has been reported to be up to 10 times as common in central European countries as in tropical countries such as Peru, Ecuador, or Panama, but data from other countries conflict with these extreme examples.
Certainly the Westemizing of the Japanese diet has provided persuasive evidence of the carcinogenic role of fat. Nutrition surveys of 1955 and 1984 indicate that the fat intake of Japanese women increased by about 180 percent during these years and the mortality from colorectal cancer increased by about 130 percent. There was a lag of about 15 years between the beginning of the widespread dietary change and the beginning of the increase in death from this neoplasm. A recent U.S. study has also demonstrated an association between a high level of animal fat consumption and the occurrence of this neoplasm. The predominant hypothesis for this association is that, since a higher fat consumption increases the excretion of bile acids and the growth of colonic bacteria, the opportunity to convert bile acids into carcinogenic substances by bacterial metabolism is facilitated. In the United States the incidence of colorectal cancer has remained stable in white men and has decreased moderately in white women, but has increased in the black population. In addition to changes in incidence, an unexplained pathological change has been occurring: In U.S. patients the lesion is less commonly located in the rectum and more commonly found in the colon. It would be satisfying to conclude that this is a reflection of the increasingly frequent removal of premalignant lesions from the rectum, but medical intervention is an unlikely explanation.
One well-recognized environmental carcinogen is the ultraviolet component of sunlight, which is a major cause of skin cancers. Susceptibility is related to paleness and a poor ability to tan, as well as to chronic exposure to sunlight. The overall incidence of nonmelanoma skin cancers in the white U.S. population is about 165 per 100,000. However, the prevalence in Texas is about three times that in Iowa. The incidence of melanoma is only about 4 per 100,000, but 65 percent of the deaths attributed to skin cancers are caused by this disease. The lesion occurs twice as often on the legs of white women as on those of white men. It occurs nearly twice as frequently on the male trunk than the female trunk. This may reflect relative exposure to sunlight due to differences in clothing. Not only is melanoma uncommon in blacks, but its location tends to be different: It is more commonly found on palms or soles and within the mouth - less heavily pigmented areas. The incidence of melanoma has been found to be increasing wherever statistics have been kept. The highest incidence has been found in Arizona (16 per 100,000), where the disease has more than quadrupled in the brief period from 1969 to 1978. It also quadrupled in Connecticut from 1939 to 1972. The smallest increase has been observed in Sweden: 80 percent from 1957 to 1971. Consistent with the increased incidence, mortality has nearly doubled. Whether the increase of this lethal disease is attributable to changes in ultraviolet intensity due to atmospheric pollution is as yet unknown.
Turning to human cancers definitely attributable to “civilization,” X-rays and related ionizing radiation are estimated to be the cause of no more than 3 percent of cancers. Exposime to radon gas has been clearly shown to be a cause of lung cancer in uranium miners. Although this is a small group at risk, if it were confirmed that the concentration of radon in some homes was sufficient to be carcinogenic, presumably the proportion of cases of cancer known to be due to radiation exposure would increase substantially. Thyroid cancer results from a small to moderate radiation exposure to the neck with a latency period of about a decade. A dose that is large enough to destroy the gland leaves no tissue to undergo neoplastic transformation. Bone marrow is another radiosensitive organ. The increased risk of developing leukemia, depending on dosage of radiation, begins as early as 2 years after exposure, reaches a peak probability after 6 to 8 years, and then diminishes. Fetuses and infants are particularly sensitive.
Suspicion of potential carcinogenesis has also fallen on synthetic food additives, such as dyes and flavoring agents, and contaminants, such as pesticides and fertilizers, either from direct spraying or from absorption of affected groundwater. Because of this suspicion, the Delaney amendment to the U.S. Food, Drug and Cosmetic Act was passed in 1958. The amendment requires the banning of food additives if they cause cancer in any species of experimental animal in any dosage. One result has been the forced withdrawal of some products based on quite dubious and unrealistic experiments. In view of the huge number of compounds, both synthetic and natural, to which people are exposed, usually in combinations having unknown interactions, deciding which ones to test and what tests are both relevant and practical is an insoluble problem.
Worldwide, stomach cancer, which has become relatively uncommon in the United States, is the most prevalent visceral cancer (second for men, fourth for women). Nevertheless, death rates have been declining since the 1930s to become only about 35 percent of what they were at that time. The decrease has been worldwide and for unexplained reasons. It remains the most prevalent carcinoma in East Asia, with the rate in Japan being more than seven times that in the United States, accounting for one-third of all cancer deaths on those islands. The repetitive ingestion of high concentrations of salt irritates the stomach lining, and this has been proposed as a potential cause of gastric cancer. In fact, the decline in the incidence of this disease has been correlated with the decline in the salt preservation of foods. In regions in which stomach cancer remains common, such as Japan, salted seafood has remained a dietary staple. The incidence of gastric cancer among first-generation immigrants from Japan to the West is similar to that in their communities of origin, but it declines to the incidence of the Western community in which the next generation resides. This suggests that the neoplastic process begins irreversibly during childhood, regardless of relocation or dietary changes after a certain age. Because this is not a genetically determined disease, a generation that has not been exposed to the inducing irritant of salt at a critical age presumably will not suffer inordinately from this neoplasm.
Carcinoma of the cervix appears not to be related to geography, but primarily to the sexual practices in a given region or subculture. The commencement of sexual intercourse during adolescence, multiple partners, or partners who have had numerous partners are all factors associated with an increased risk of developing the disease, as is a large number of pregnancies. Thus, carcinoma of the cervix is rare among nuns and common among prostitutes. A sexually transmitted virus is suspected to be a causative factor or cofactor. As with prostatic cancer, chronic cigarette smoking appears to increase the risk of occurrence of this neoplasm. Another peculiar difference, at least in the United States, is that carcinoma of the cervix occurs about twice as frequently among black as among white women, whereas carcinoma of the uterus occurs two to four times as often in white women.
Cancer of the liver is much more prevalent in many of the developing countries than in the industrialized world. Its incidence is highest in subSaharan Africa, China, southern Asia, and Japan (the exception among industrialized countries). China alone accounts for about 45 percent of the world’s cases. The liver is subject to two principal types of cancer. One originates in liver cells, and a history of infection with the hepatitis B virus predisposes to this. The other originates in cells of the bile ducts. A predisposition to develop this form of cancer is caused by infestation with the liver fluke Clonorchis sinensis and related parasites. The geographic distribution of these parasites is reflected in the prevalence of this disease. Alcoholism has not been shown to be a major predisposing factor.
Other cancers in the developing world are associated with indigenous infectious agents and with cultural practices. Betel nut chewing, for example, is linked with high rates of oral cancer in central and southeast Asia and Kashmir; Bantu natives, who hold warming pans of charcoal against their bodies, are subject to cancers of the abdominal wall. The frequent occurrence of esophageal cancer has been related to the consumption of very hot beverages in some cultures. Burkitt’s lymphoma, which occurs almost exclusively in central Africa and New Guinea, is probably caused by the Epstein-Barr virus in genetically predisposed individuals. Bladder cancer is a common problem in North Africa, and especially Egypt, because infestation with the parasite Schistosoma haematobium induces the disease.
In summary, the concept of cancer has evolved through the ages from that of a single disease to one of many diseases with many causes. Most prevalent are carcinomas of the stomach, lungs, breast, cervix, colon and rectum, prostate, and liver. Chief among carcinogens are irritants such as fumes of tobacco and certain metals, ionizing and ultraviolet radiation, specific chemical compounds, some helminthic parasites, and possibly viruses. Everyone is constantly bombarded by carcinogens of various potencies, but cancer develops in a minority of people. A few uncommon neoplasms clearly are genetically determined, but the degree of resistance to carcinogens also appears to have a genetic basis.
Yet even if cancer is viewed as multiple diseases with multiple causes, each disease involves the same phenomenon: an inadequately controlled division and multiplication of cells that can infiltrate adjacent tissues and, in many types, form distant secondary lesions. The factors that permit metastatic tumor cells to survive and implant remain just as mysterious as the factors that initiate the loss of control of cell division.
The available treatments are generally drastic and poorly selective of the foci of disease and, in many circumstances, not curative. Earlier diagnosis improves the cure rate of many but not all cancers. Therefore, public education about the signs of cancer and further improvements in the sensitivity of diagnostic methods should be sought. However, until our Imderstanding of the fundamental biology of cancer improves, preventive measures, such as minimizing exposure to known carcinogens, will exert by far the greatest benefit to public health.
Thomas G. Benedek and Kenneth F. Kiple
Bibliography
Ackerknecht, Erwin H. 1965. History and geography of the most important diseases. New York.
Austoker, Joan. 1988. A history of the Imperial Cancer Research Fund. Oxford.
Boyle, P., C. S. Muir, and E. Grundmann, eds. 1989. Cancer mapping. New York.
Braun, Armin C. 1977. TAe story of cancer: On its nature, causes, and control. London.
Burnet, Macfarlane, and David O. White. 1972. Natural history of infectious diseases, 4th edition. Cambridge.
Cancer Research Campaign. 1988. Factsheet, Nos. 4-12. London.
Davis, Devra Lee. 1989. Natural anticarcinogens, carcinogens, and changing patterns in cancer: Some speculation. Environmental Research 50: 322-40.
Doll, R., and A. B. Hill. 1952. A study of the aetiology of carcinoma of the lung. British Medical Journal. 2: 1271-86.
1954. The mortality of doctors in relation to their smoking habits. British Medical Journal 1: 1451-5.
Doll, R., and R. Peto. 1976. Mortality in relation to smoking: 20 years’ observations on male British doctors. British Medical Journal 2: 1525—30.
1981. The causes of cancer: Quantitative estimates of avoidable risks of cancer in the United States today. Oxford.
Elwood, J. M., and J. A. Lee. 1975. Recent data on the epidemiology of malignant melanoma. Seminars in Oncology 2: 149-53.
Emster, V. L. 1988. Trends in smoking, cancer risk, and cigarette promotion. Cancer 62: 1702—12.
Greenberg, Michael. 1983. Urbanization and cancer mortality: The United States experience, 1950-1975. New York.
Haenszel, W., and M. Kurihara. 1968. Studies of Japanese migrants. I. Mortality from cancer and other diseases among Japanese in the United States. Journal of the National Cancer Institute 40: 43—68.
Hammond, E. C., and D. Hom. 1958. Smoking and death rates: Report on forty-four months of follow-up of 187,783 men. Journal of the American Medical Association 166: 1159-72.
Hirsch, August. 1886. Handbook Ofgeographical and historical pathology, Vol. 3, trans. Charles Creighton. London.
Hippocrates. 1931. Aphorisms VI, trans, and ed. W. H. S. Jones. Cambridge.
Honda, G. D., L. Bemstein, R. K. Ross, et al. 1988. Vasectomy, cigarette smoking, and age at first sexual intercourse as risk factors for prostate cancer in middle-aged men. British Journal of Cancer 46: 1307-18.
Howe, G. Melvyn. 1977. A world geography of human diseases. London.
Jones, Lovell A., ed. 1989. Minorities and cancer. New York.
Luinsky, William. 1989. Environmental cancer risks - real and unreal. Environmental Research 50: 207-9.
McGrew, Roderick E. 1985. Encyclopedia of medical history. New York.
Miller, D. G. 1980. On the nature of susceptibility to cancer. Cancer 46: 1307—18.
Mills, P. K. et al. 1989. Cohort study of diet, lifestyle, and prostate cancer in Adventist men. Cancer 63:598-604.
Muir, C. S. 1990. Epidemiology, basic science, and the prevention of cancer: Implications for the future. Cancer Research 50: 6441—8.
Natarajan, N., G. P. Murphy, and C. Mettlin. 1989. Prostate cancer in blacks: An update from the American College of Surgeons’ patterns of care studies. Journal of Surgical Oncology 40: 232—6.
Parkin, D. M., E. Laara, and C. S. Muir. 1988. Estimates of the worldwide frequency of sixteen major cancers in 1980. International Journal of Cancer 41: 184-97.
Patterson, James T. 1987. The dread disease: Cancer and modern American culture. Cambridge, Mass.
Preston-Martin, S., et al. 1990. Increased cell division as a cause of human cancer. Cancer Research 50: 7415-21.
Rather, L. J. 1978. The genesis of cancer: A study in the history of ideas. Baltimore.
Reedy, J. 1975. Galen on cancer and related diseases. Clio Medica 10: 227-38.
Satariano, W. A., and M. Swanson. 1988. Racial differences in cancer incidence: The significance of agespecific patterns. Cancer 62: 2640-53.
Silverberg, E., C. C. Boring, and T. S. Squires. 1990. Cancer statistics, 1990. California Cancer Journal for Clinicians 40: 9-25.
Swanson, G. M. 1988. Cancer prevention in the workplace and natural environment. Cancer 62: 1725-46.
Whittemore, A. S., and A. McMillan. 1983. Lung cancer mortality among U.S. uranium miners: A reappraisal. Journal of the National Cancer Institute 71: 489-505.
Willett, W 1989. The search for the causes of breast and colon cancer. Nature 338: 389-94.
Willett, W, et al. 1990. Relation of meat, fat, and fiber intake to the risk of colon cancer in a prospective study among women. New England Journal of Medicine 323: 1644-72.
Wolff, Jacob. 1907. The science of cancerous disease from earliest times to the present, trans. Barbara Ayoub, 1989. Canton, Mass.
United States General Accounting Office. 1987. Cancer patient survival: Whatprogress has been made? Washington, D.C.
Zarizde, S., and P. Boyle. 1987. Cancer of the prostate: Epidemiology and aetiology. British Journal of Urology 59: 493—502.