Quality of Life
Mortality rates and other statistics derived from them imply that we have measures for the number of years survived. Yet equally measured mortality levels may represent quite different qualitative experiences.
In search of ways to capture the quality of life, researchers have selected mortality indexes believed to be more revealing, such as infant or maternal mortality, and have combined vital and economic statistics. One index, used widely to compare the quality of life in Third World countries, is the Physical Quality of Life Index, which uses a weighted average of several demographic and economic statistics (Morris 1979). It has some possibilities for application to historical societies for which equivalent data are available.A more promising approach to the quality of life draws on health statistics. Unlike mortality, ill health - morbidity - is not an unambiguous quantity. Individuals and societies make different decisions about the threshold between health and ill health, and these decisions raise problems concerning definitions and measurements of ill health. Some standard gauges rely on diagnostic evidence; these are encountered in reports of the number of cases of specific diseases identified in a given region and period. Other gauges are based on contact with health institutions or personnel (hospitalizations, physician visits). Still others depend on evidence about individual performance, such as restricted activity, bed disability, or work time lost; these measures are often encountered in insurance records and health surveys. Because different sources provide different forms of evidence, the important point is to find a gauge whose definition is consistent (Riley 1989).
Morbidity also differs from mortality in its complexity. Different questions are at issue. A morbidity rate may express the number of times members of a population fall ill during a period (incidence), the proportion of the population ill at a given time (prevalence), or the amount of time spent in illness by a population during a given period (duration).
To take only the two extreme cases - incidence and duration - the age-specific risk of falling sick (incidence) is concave and resembles the inside of a shallow bowl, and that of being sick (duration) looks like the misshapen W identified earlier. Figure IV.4.3 provides examples of these morbidity curves, using Friendly Society records from nineteenth-century Britain (Riley 1987). Like the mortality schedule, the morbidity schedule may move up or down over time, a factor influenced by objective health experience and by subjective decisions about the threshold between health and ill health. Individual curves are likely to vary from these forms, especially when the characteristics of the population under observation change over time. For example, the National Health Interview Survey shows a morbidity schedule with a slower rate of increase at higher ages, a factor attributable in part to the exclusion of institutionalized members of the population from the survey (National Center for Health Statistics). More investigations of health experience in historical societies will help identify the causes of variation (Larsen 1979; Beier 1985; Pelling 1985).Morbidity rates in turn can be used in association
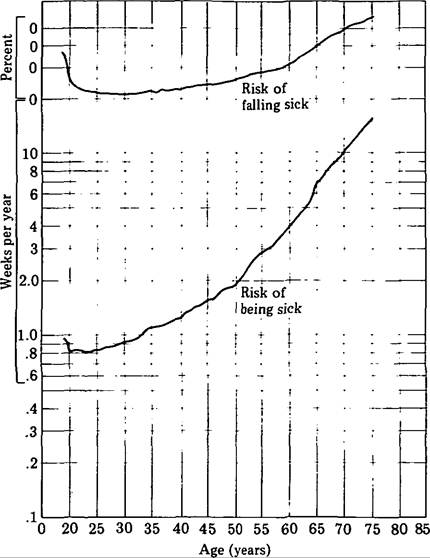
Figure IV.4.3. Morbidity rates for nineteenth-century
Britain. (From Nelson 1982.)
with mortality rates to estimate the number of ill- health episodes to be expected in the average remaining lifetime or, alternatively, the proportion of lifetime remaining to be spent in ill or good health. The technique makes use of age-specific morbidity rates in combination with mortality risks in the life table. The health expectation, sometimes called the active life expectation, uses the age-specific risks of mortality and being sick to estimate the remaining lifetime and the portion of that time to be spent in good health (Riley 1989).
If changes in ill-health rates paralleled those in mortality rates, the two rising or falling together, then morbidity risks and health expectation could be estimated from mortality risks.
But investigation of the association between mortality and morbidity suggests that the straightforward form of this tie - deaths are attributed to ill health - belies the statistical and population-level associations. Rates of falling sick and being sick change independently of mortality rates, which is to say that the risk of dying once one is sick changes over time. The association is conditioned by environmental forces, such as therapeutic regime or standard of living, and by changes in the composition of the population that can be attributed to mortality. For example, insurance records and health surveys show that the mortality decline of the twentieth century has been accompanied by increased duration of ill health at each age (Alter and Riley 1989).In other words, the proportion of people dying from a given disease or injury - the case fatality rate - has shifted. Changes have occurred in the percentage of people surviving, a concept dramatically illustrated by the history of diseases that vary in virulence or that cause death much more often among people with no prior contact with them than among people relatively resistant to them, and familiar also in terms of changes in the efficacy of therapies. The case fatality rate is a useful way to measure the severity of diseases that have a short course. For chronic diseases, however, it is necessary to consider the prolonged duration of an ailment and the likelihood of death from another cause during its course. A related notion, which might be termed case duration, is the time between onset and resolution. That period may change as diagnostic practices shift or as a population’s view of the ill-health threshold or its recognition of ill- health episodes changes. And it may also shift when new therapies are introduced. Because, with notable exceptions, case fatality rates as high as 50 percent have been rare, it is apparent that most ill- health episodes are resolved in recovery. Even in acute diseases, duration has been an important element in the disabling effects of illness, injury, and collective violence.