100 Paget’s Disease of Bone
Paget’s disease of bone was described as “osteitis deformans,” a “chronic inflammation of bone” by Sir James Paget in an address to the Royal Medical Chirurgical Society of London in 1876.
His original description was masterful and thus has withstood the test of time. Paget’s disease of bone describes an abnormal osseous (bony) structure whereby isolated and sometimes contiguous areas of the skeleton undergo changes leading to clinical deformity for some of those affected. Clinically affected people may have the appearance of enlarged bone, bowed extremities, shortened stature, and simian posturing because the body’s usual system for maintaining strong and healthy bone malfunctions. Normal bone turnover is altered in the affected areas. The resorption process accelerates, and the repair process responds by building a heavy, thickened, and enlarged bone. Although the new bone contains normal or increased amounts of calcium, the material of the bone is disorganized, and the bone is structurally weak. The result may be pain, deformity, fracture, and arthritis.
Distribution and Incidence
The disease appears to have its greatest prevalence in Europe and in regions inhabited by European emigrants such as Australia, New Zealand, and areas of South America. For no apparent reason, the disease is distinctly uncommon in African blacks, Orientals, and inhabitants of India and Scandinavia. Where studied, the incidence ranges between 3.5 and 4.5 percent of the population in high prevalence regions of the world, with a high of 8.3 percent in a part of Lancashire, England, to a low of 0.4 percent in Sweden. In a U.S. survey of Paget’s disease based on pelvic X-rays, the incidence was 3.9 percent in Caucasians residing in Brooklyn and 0.9 percent in Caucasians residing in Atlanta. Similarly, 1,000 pelvic X-rays revealed no Paget’s disease in Lexington, Kentucky, and 1.1 percent pelvic Paget’s disease in Providence, Rhode Island.
Epidemiology and Etiology
Males are more at risk from Paget’s disease than are females by a 3:2 ratio. There is evidence Ofheritabil- ity: A survey, for example, revealed that 13.8 percent of patients with Paget’s disease had relatives
with Paget’s disease. Approximately half were from successive generations and half from siblings. Familial cases had an earlier onset than did isolated cases. An autosomal dominant pattern was suggested.
The etiology remains unknown. Paget named this disease “osteitis deformans” in the belief that the basic process was inflammatory and had an infectious origin. Recent Ultrastructural studies of involved bone have revealed nuclear and cytoplasmic inclusions. They have not been found in bone cells of patients with other skeletal disorders, with the exception of giant cell tumors of bone. Morphologically the nuclei resemble those of cells infected with paramyxoviruses such as parainfluenza, mumps, and measles, and the cells resemble cultured cells infected with respiratory syncytial virus (RSV).
This tubular morphological finding has raised the question as to whether Paget’s disease is a slow virus infection of bone. Other slow virus infections of human beings have similarly demonstrated a long clinical latent period, absence of an acute inflammatory response, a slowly progressive course, restriction of disease to a single organ system, patchy distribution in the body, and genetic predisposition.
Immunohistological studies of bone biopsy specimens have demonstrated antigen from RSV and measles. An indirect immunofluorescence antibody assay has demonstrated evidence for both measles and RSV antigens in Pagetic bone grown in culture from 30 patients. The suggestion of different RNA viruses (measles is a member of the genus Morbillivirus, whereas RSV is a member of the genus Pneumovirus) seems incompatible. It has been proposed that Paget’s disease stems from a previously uncharacterized virus, perhaps of the Pneumovirus group.
According to this hypothesis, Paget’s disease patients are infected with a slow virus at an early age, probably under the age of 30. The slow virus isolates to particular areas of the skeleton by growth pattern and/or blood supply. As the metabolic activity of the skeleton decreases with age, the infested osteoclasts increase their metabolic activity, eventually producing diseased bone some 20 to 40 years following the initial infestation.Clinical Manifestations
It is estimated that 80 percent of people with Paget’s disease are asymptomatic and have no clinical findings suggestive of the disease. When symptomatic, the clinical manifestations are often defined by the complications of the disease. Clinical findings may include some or all of the following: frontal bossing, scalp vein dilatation, angioid streaks, simian pos-
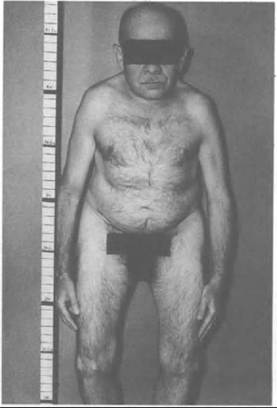
Figure VIIL 100.1. Severe Paget’s disease of the bone in a 66-year-old male. Note the anthropoid appearance and simian posturing, with the anterior and lateral bow to the arms, thighs, and legs. There are functional flexion contractures of the hips and knees.
ture, short stature, flexion contractures at hips and knees, anterior and lateral bowing of long bones, warmth of involved extremity, periosteal tenderness, and compressive neuropathy. Figure VIIL 100.1 shows a man with severe Paget’s disease of bone.
Pagetic bone pain is uncommon, but when present it is aching, deep, poorly described, and occasionally continuous at night. It is often aggravated by pressure or weight bearing.
The following deformities may develop: (1) The involved skull may become soft, thickened, and enlarged; (2) the femora tend to migrate medially and superiorly deforming the softened pelvis; (3) enlargement of vertebrae alters the spine, resulting in an anthropoid appearance; (4) the affected long bones soften and bow from weight-bearing or from the force of the surrounding muscles.
Pathological fractures can also occur in the form of compression fractures of vertebrae, incomplete or stress fractures of the long bones, or completed fractures of long bones.
The relation of secondary osteoarthritis to Paget’s disease has recently been emphasized. Low back pain is the most common clinical presentation of Paget’s disease and is often related to secondary osteoarthritis.
Sarcomatous degeneration, although uncommon, does occur in approximately 1 percent of patients with Paget’s disease, representing a 40-fold increase over that of the general adult population. It is most often heralded by increasing pain.
Skull symptoms may include headaches, vertigo, rushing sensations, and noise in the head. Maxillary exceeds mandibular involvement by a 2:1 ratio, and both may disrupt the lamina dura or cause unsightly deformity. Hearing loss may be severe but is most often moderate.
Neural compression may occur from spinal stenosis or a spinal lateral recess syndrome. Paraparesis - paraplegia in Paget’s disease - is most often related to Paget’s disease of dorsal or cervical vertebrae.
History and Geography
Paget’s disease is not a new disease, having been suspected in a Neanderthal skull. Although isolated case reports in the mid-nineteenth century describe what is now called Paget’s disease, the classical clinical description by Paget and a pathological description by Henry Butlin clarified this entity in 1876. Paget was a major figure in the medical community, having been knighted at the age of 43, at which time he began his observations of the first patient with the bone disease that would bear his name. He is also credited with having defined such diseases as Paget’s disease of the breast, rectum, and skin; carpal tunnel syndrome; and trichinosis. Paget’s disease of bone is unique in that it affects only adult humans; reports of Paget’s disease in animals are not convincing. A childhood osseous condition called juvenile Paget’s disease appears to be a separate entity.
At present, it is difficult to reconcile the geographic isolation of this disease to Europeans (exclusive of Scandinavians) and their descendants.
Theories of a slow virus infection in susceptible individuals seem dubious, for if this were the case, then theoretically the disease would have a more worldwide distribution. Isolated case reports of Paget’s disease in South African blacks, Japanese, and Indians (from India) only serve to confuse the issue of transmission.Temperature cannot be implicated, as high prevalence areas include disparate climatic regions of Italy, Spain, Germany, and eastern Russia. Similarly, occupation and degree of physical activity do not appear related to the cause of Paget’s disease as the blend of geographic areas involves all types of lifestyles. Interestingly, the black population of the United States appears to sustain a higher frequency of Paget’s disease than might be expected, given the rarity of the disease in Africa. An explanation in part involves intermarriage with those of European ancestry.
Roy D. Altman
Bibliography
Altman, R. D., and B. Collins. 1980. Musculoskeletal manifestations of Paget’s disease of bone. Arthritis and Rheumatism 23:1121-7.
Altman, R. D., and R. Winchester. HLF-A, B, C, D, Dr loci in Paget’s disease. School of Medicine, University of Miami. Miami, Fla. (Unpublished data.)
Barry, H. C. 1969. Paget’s disease of bone. Edinburgh and London.
Cullen, P., et al. 1976. Frequencies of HLA-A and HLA-B: Histocompatibility antigens in Paget’s disease of bone. Tissue Antigens 7: 55-6.
Dickson, D. D., et al. 1945. Osteitis deformans: Paget’s disease of bone. Radiology 44: 449-70.
Fotino, M., et al. 1977. Evidence for linkage between HLA and Paget’s disease. Transplant Proceedings 9: 1867-8.
Howatson, A. F., and V. L. Fomasier. 1982. Microfilaments associated with Paget’s disease of bone: Comparison with nucleocapsids of measles virus and respiratory syncytial virus. Intervirology 18: 150-9.
Mills, B. J., et al. 1980. Cell cultures form bone affected by Paget’s disease. Arthritis and Rheumatism 23: 1115-20.
1984. Evidence for both respiratory syncytial virus and measles virus antigens in the osteoclasts of patients with Paget’s disease of bone.
Clinical Orthopaedics OndRelatedResearch 183: 303-11.Morales, A., et al. 1980. Manifestaciones articulares de la enfermedad de Paget. Revisibn de 84 casos. Revista Cltnica Espahola 159: 195—8.
Paget, J. 1877. On a form of chronic inflammation of bones (osteitis deformans). Medico-Chirurgical Transactions 60: 37—64.
Rebel, A., et al. 1974. Particularites Ultrastructuales des Osteoclastes de la maladie de Paget. Revue du Rhumatisme et des Maladies Osteo-articulaires 41: 767-71.
1980. Viral antigens in osteoclasts from Paget’s disease of bone. Lancet 2: 344-6.
Rosenbaum, H. D., and D. J. Hanson. 1969. Geographic variation in the prevalence of Paget’s disease of bone. Radiology 92: 959-63.
Sofaer1 J. A., et al. 1983. A family study of Paget’s disease of bone. Journal of Epidemiology and Community Health 37: 226-31.
Tilyard, M. W., et al. 1982. A probable linkage between familial Paget’s disease and the HLA loci. Australian and New Zealand Journal OfMedicine 12: 498—500.