153 Typhus, Scrub (Tsutsugamushi)
Tsutsugamushi, like epidemic typhus, has been known in the Orient for centuries. In 1810 the Japanese Hakuju Hashimoto described a tsutsuga (disease) along the tributaries of the Shinano River.
A similar disease, thought to be carried by mites, or mushi in Japanese, had also been known at least since the sixteenth century in southern China. Sometimes called Japanese flood fever, tsutsugamushi is more commonly known in the United States as scrub typhus —a name used widely by English-speaking troops during World War II. The disease exhibits characteristic typhuslike symptoms of high fever, headache, duration of 2 weeks, and a widespread rash.Distribution and Incidence
The geographic boundaries of this malady are defined by the range of its vectors, primarily the trombiculid mites, Lentotrombidium akamushi and Leototrombidium deliensis, and their vertebrate hosts. They extend from India and Pakistan in the West, to Japan and the northern portions of Australia, including all the countries of Southeast Asia, southern China, Korea, the Philippines, and Indonesia, as well as additional islands in the Pacific Ocean (see Map VIII. 153.1). During World War II, the incidence of scrub typhus rose dramatically among military troops, reaching 900 per 1,000 personnel in some areas. It continues to remain a problem in isolated, rural areas.
Etiology and Epidemiology
The etiologic agent of scrub typhus, R ickettsia tsutsugamushi, is a natural infection of several trombiculid mites, most commonly L. deliensis. Maintained in nature by generational transmission through the eggs of the female, the disease is communicated to humans only during the larval stage of the mite’s life cycle. At this time, the six-legged larval mite, often called a “chigger,” seeks an animal on which to find a meal of tissue juices, or lymph. Usually they feed on field mice, rats, tree-shrews, and other small mammals, but humans are satisfactory if they happen into the mite’s environment.
Ground-frequenting birds may also become infected and transport infected mites to a new location. In later stages of their lives, the mites live in the soil and not in animals.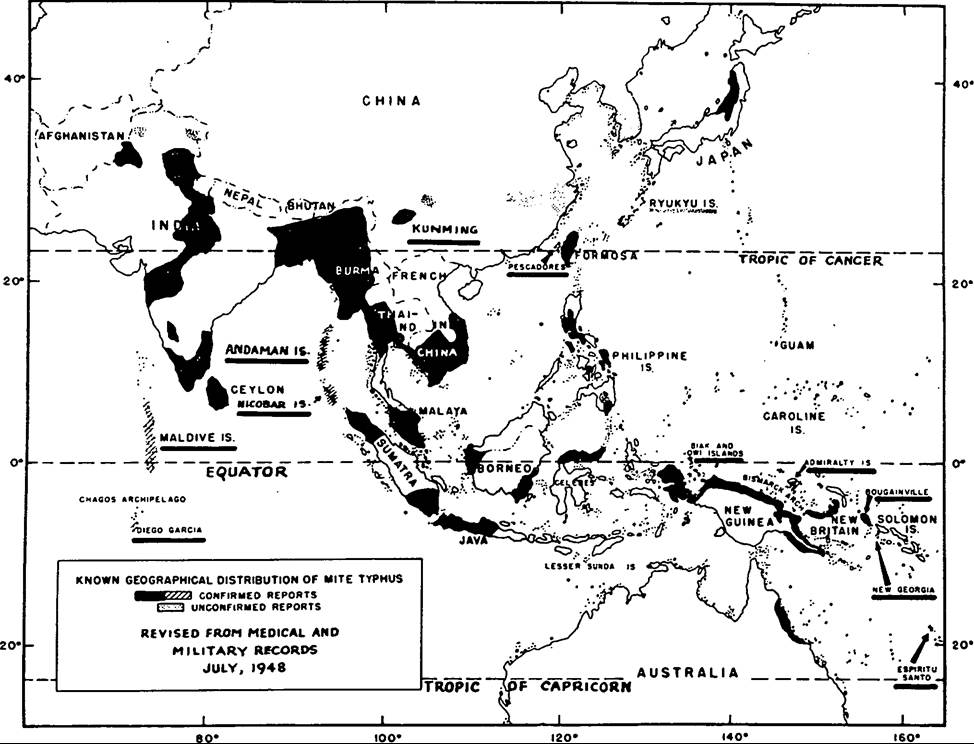
Map VΠI.153.1. Known geographic distribution of mite (scrub) typhus in Asia, July 1948.
Because of the wide geographic area across which tsutsugamushi is spread, its epidemiological pattern varies. In the Niigata region of Japan, for example, the disease is most common during the summer months, associated with increased incidence of the mite L. akamushi, whereas in the Chiba and the Kanagawa prefectures and the Izu Schichito Islands, it occurs in mild form throughout autumn and winter. In Malaya, a hot, tropical climate supports the disease throughout the year, and near the India- Burma border it is usually associated with the monsoon season.
Similarly, a variety of terrains may support the development of the vector mites, including grassy fields, river banks, neglected or abandoned rice fields, overgrown clearings, forests, jungles, and border areas between field and forest. The key requirements in any area include a suitable rodent population and sufficient ground moisture to support the mites. The “islands of infection” in which scrub typhus typically occurs apparently represent favorable ecological conditions for the mites.
Clinical Manifestations
Scrub typhus incubates in human hosts for about 10 to 12 days, after which it manifests itself suddenly, with chills and fever, headache, and other typical typhuslike symptoms. In most Caucasians and, less frequently, in Asians, an eschar or initial lesion from the mite bite occurs and causes lymph-gland swelling. During the first week of the disease, the fever increases to 104o or 105oF. Between the fifth and the eighth day, a red macular rash appears on the trunk of the body, and it may extend to the arms and the legs.
During the second week, the pulse rate may increase to 120 or 140, blood pressure falls, and neurological symptoms such as deafness, stupor, delirium, and muscle twitching may appear in untreated patients. Pneumonia and signs of circulatory failure may also occur, but by the beginning of the third week, those untreated individuals who recover begin to experience a reduction in fever and other symptoms. Those who die usually do so by the end of the second week from circulatory failure or from secondary pneumonia or encephalitis. Even in recovered patients, however, neurological effects may continue, and convalescence is usually long. Fortunately, the broad-spectrum antibiotics have reduced the mortality in treated patients to nearly zero.Unfortunately, the immunity conferred by this infection is specific to the scrub typhus strain only. Current infections may occur when the individual is infected by other strains.
History and Geography
Reports of tsutsugamushi reach back to at least the sixteenth century in the Orient. Bacteriologic investigations of the disease began in Japan in the early 1890s when it captured the attention of Shibasa- buro Kitasato, who had returned from his work with Robert Koch in Germany to found the Institute for Infectious Diseases in Tokyo. Various other researchers, principally Japanese, continued to study the disease through the first three decades of the twentieth century, identifying its causative microbe as a rickettsiae.
Renewed investigation by Western scientists was stimulated by severe outbreaks of scrub typhus in the Pacific and the China-Burma-India theaters during World War II. With the Allied countermove to stem the rapid Japanese advance in the Pacific, the occupation of islands often took place in haste, and groups of soldiers would shortly become very ill. Between January 1943 and August 1945, scrub typhus disabled some 18,000 Allied troops, including 6,685 American servicemen. Fatality rates varied from a low of 0.6 percent in some regions to as high as 35 percent in others; there were 234 deaths among U.S.
troops.Throughout the 1920s and 1930s, British researchers and their colleagues at the Institute of Medical Research in Kuala Lumpur, Federated Malay States, had observed that tsutsugamushi was distinguished from other typhuslike diseases by its reaction to a particular strain of bacteria used in the Weil-Felix test. When the U.S. Typhus Commission began to study scrub typhus (“because of its last name” as Commission Director Stanhope Bayne- Jones noted) the Weil-Felix diagnostic test was virtually the only laboratory tool available. Numerous experts in medicine, epidemiology, and entomology were called upon to examine the problem, and, by the end of the war, two major lines of defense against the disease had been developed.
The first was prevention. The army launched education efforts, including posters describing the mite, where it was likely to be found, and how soldiers should prepare their campsites to avoid it. In addition, chemicals were developed to impregnate clothing that would repel the tsutsugamushi mite. Benzyl benzoate proved to be effective and lasted 2 weeks before reapplication was necessary. The second line of defense focused on intensive research to develop an antiserum or a vaccine against tsutsugamushi. World War II ended, however, before either could be made practical. In 1948, the broad-spectrum antibiotic chloramphenicol was tested at the Institute of Medical Research in Kuala Lumpur and found to be highly effective as treatment for the disease.
Victoria A. Harden
Bibliography
Blake, Francis G., et al. 1945. Studies on tsutsugamushi disease (scrub typhus, mite-bom typhus) in New Guinea and adjacent islands: Epidemiology, clinical observations, and etiology in the Dobadura area. American Journal of Hygiene 41: 243-372.
Kawamura, Rinya. 1926. Studies on tsutsugamushi disease (Japanese flood fever). Bulletin of the College of Medicine of the University OfCincinnati 4 (special Nos. 1 and 2): 1-229.
Philip, Cornelius B. 1964. Scrub typhus and scrub itch. In Preventive medicine in World WarII, Vol. 7: Communicable diseases: Arthropodborne diseases other than malaria, 275-347. Medical Department, U.S. Army.
Santana, Frederick J., et al. 1976. Annotated bibliography of scrub typhus in Taiwan and the Pescadores Islands (1911—1975). A special publication of U.S. Naval Medical Research Unit No. 2. Taipei, Taiwan.
Smadel, Joseph E., and Bennett L. Elisberg. 1965. Scrub typhus rickettsia. In Viral and rickettsial infections of man, 4th edition, ed. Frank L. Horsfall, Jr., and Igor Tamm, 1130—43. Philadelphia.