154 Urolithiasis (Renal and Urinary Bladder Stone Disease)
The major forms of urolithiasis consist of either upper tract stones within the kidneys or ureters (renal stones) or lower tract stones formed within the bladder. These two forms of urolithiasis have distinct differences in etiology, chemical composition, and epidemiological features, and should therefore be considered two separate diseases.
Historical evidence has shown a striking increase in incidence of renal stone disease in more developed countries over the past 100 years. There has been a simultaneous decrease in bladder stone incidence, demonstrating an inverse relationship between the two disorders. Changes in the environment have a profound effect on the epidemiology of human diseases. An unusual example of this interplay is the role of dietary change in the shifting epidemiological pattern from bladder stone to renal stone disease.
Etiology
The large majority of bladder stones occur in young boys from rural or impoverished areas. In these regions, the disorder is known as endemic bladder stone disease. Information from both historical and experimental sources points to a nutritional deficiency during infancy or possibly in utero as the major factor in endemic bladder stone formation. Other less common causes of bladder stone are schistosomiasis (producing bladder wall thickening, stricture, and outlet obstruction) as well as obstruction in elderly males from benign prostatic hypertrophy.
Although deficiencies of vitamin A, vitamin B6, or magnesium have been suggested in endemic bladder stone disease, low intake of animal protein in combination with high intake of grain carbohydrate is more important. Indeed, it seems that whereas low animal protein intake in infancy may cause bladder stone, a high animal protein diet provokes renal stones (Robertson 1978). This probably explains the epidemiological enigma of the disappearance of endemic bladder stone as areas improved economically, with a concomitant increasing incidence of renal stone (Table VIII.
154.1).Low intake of animal protein and high intake of grain carbohydrate produce more acidic urine and decreased urinary phosphate excretion. These in turn Table VIΠ. 154.1. Major features differentiating bladder and renal stone disease
| Features | Bladder stone | Renal stone |
| Age | Young children | Adults |
| MZF ratio | 12:1 | 1.2:1 |
| Socioeconomic | Poor, usually ru- | All classes affected |
| class | ral areas | in more developed countries |
| Diet | Almost strictly vegetarian; animal protein intake 40 g; high intake of refined sugar | |
| Chemical | Ammonium acid | Calcium phosphate, |
| composition | urate, uric acid, calcium oxalate | calcium oxalate, other |
| Recurrence | Rare | Frequent |
decrease the solubility of calcium oxalate and uric acid leading to bladder stone formation. Conversely, greater animal protein intake produces more urinary phosphate. An increased intake of refined sugar plus a decreased intake of fiber increase the intestinal absorption of calcium. Increased protein and sucrose intake cause increased urinary calcium excretion, possibly secondary to a distal renal tubular acidosis. This sets the stage for calcium phosphate or calcium oxalate stone formation in the kidneys.
Other less common types of renal stones have specific etiologies. For example, cysteine stones are created by a genetic defect in renal tubule reabsorption of certain amino acids.
Repeated urinary infections can result in magnesium ammonium phosphate stones. A number of systemic diseases can cause hypercalcemia with subsequent calcium stone formation. These include hyperparathyroidism and Cushing’s syndrome.Finally, a multitude of other factors also operate in renal stone formation or prevention. Substances known as stone inhibitors are normally present in the urine. Dehydration, by producing relative stasis and more concentrated urine, is an added factor in stone formation and partially explains the increased incidence in hot and arid climates and seasonal increases during summer months.
Epidemiology and Geographic Distribution
Bladder Stone Disease
Among early authors, Galen during the second century in Rome and Albucasis during the eleventh century in Spain observed the frequent occurrence of bladder stone in young boys. Bladder stone still primarily affects boys under 10 years of age. Among approximately 7,000 cases from Thailand, the median age at operation was 4.5 years. Almost 95 percent of all patients were male (Halstead 1961). Numerous clinical studies of the disease in other regions confirm the occurrence at an early age and a marked predominance of male patients (Thomson 1921; Racic 1935; Brown and Brown 1941; Eckstein 1961).
Anatomic differences in the urethra of males and females probably account for the infrequency of bladder stone in females. The female urethra is short, wide, and straight, allowing stronger flow of urine and passage of gravel before large stones are formed.
Bladder stone disease occurs in agricultural regions, particularly in the lower economic classes. Fifty years ago, bladder stone commonly occurred in the inland districts of the Balkans, where living conditions were very primitive. At the same time, the disease was rare along the Adriatic coast, where better Iivingconditionsprevailed (Anderson 1972). Bladder stone was quite common in the economically depressed rural areas of Norfolk, England, during the eighteenth and nineteenth centuries, whereas the disease was rare among the more affluent people living in the adjacent urban centers (Thomas 1949; Batty Shaw 1970).
A similar disparity is seen today between the rural farmers and city dwellers of Thailand and northern India (Halstead 1961; Anderson 1969, 1972).Accurate figures on the prevalence of bladder stone disease come from northeast Thailand, where over 20,000 people were interviewed. A history of past or present bladder stone was obtained in 3.8 percent. A small group (0.33 percent) had required surgical removal of the bladder stone (Halstead and Valyasevi 1967). Contrary to this low number, nearly 2 percent of all admissions to the Norfolk and Norwich Hospital during the period 1772-1816 were for removal of bladder stone (Batty Shaw 1970).
Historical accounts from the 1500s to the mid- 1800s document the prevalence of the disease throughout Europe, Asia, and America (Anderson 1962; Lonsdale and Mason 1966; Batty Shaw 1970; Prien 1971). Bladder stone remains quite common in Egypt, northwest India, southern China, Thailand, Afghanistan, Iraq, Turkey, and Madagascar. Prior to 1940, bladder stone was also common in portions of Iceland, Russia, Hungary, Indonesia, Tunisia, and Sicily.
Renal Stone Disease
Renal stone disease has mainly been an affliction of the more industrialized and affluent countries of Europe, North America, and Japan and has been uncommon or unknown in impoverished regions and primitive societies. However, people in these areas have developed a similar prevalence with improvement in living conditions and subsequent dietary changes (Modlin 1967).
Population studies in both America and Europe reveal prevalence rates for renal stone ranging from 3 to 13 percent. Nearly 75 percent of these people with so-called idiopathic calcium stone disease have one or more recurrences, implying a continuous exposure to risk factors such as diet. The incidence of the disease has risen continuously since the turn of the century except for brief declines during both world wars - again pointing to dietary changes as an important factor.
Unlike bladder stone disease, renal stones occur predominantly in adults.
Men are affected slightly more often than women.History and Paleopathology
Epidemiological studies have shown that bladder stone is a disease of communities where the diet is high in grain or rice and low in animal protein. With dietary changes resulting from improved technology, migration, or cultural shift, bladder stone disease is replaced by renal stone disease. This is well demonstrated over the past two centuries in parts of Britain, France and other European countries, Russia, China, and Turkey. It is therefore not surprising that ancient references to stone disease deal almost entirely with bladder stone, with rare mention of the renal colic characteristic of upper tract stones.
Bladder stone was common in ancient Persia (600-300 B.C.), particularly in infants, and was considered a result of ingesting sour milk, fruits, or acidic drinks. The Babylonian Talmud contains references to bladder stone disease and includes the ingenious suggestion that patients should urinate on the doorstep in order to see the stone.
In India, the Rig Veda and Atharva Veda, inscribed around 1500 B.C., consist of incantations against disease, including bladder stone. The Ayur Veda, published much later, around the first century A.D., described suprapubic incision for removing bladder stones. In the second century A.D., Charaka described four types of stones, almost certainly originating in the bladder. The first was white and as large as a hen’s egg; the second was rough and covered with spines; the third was of a dark color; and the fourth was composed of sperm. The first three stones were probably urate and calcium oxalate bladder stones typical of endemic disease.
Early Chinese literature contains few references to any recognizable disease. However, detailed case histories of 25 patients treated by Shunyii I in the second century B.C. have been preserved. They include a palace superintendent afflicted with hematuria, urinary retention, and bladder stones.
This may represent a case of either schistosomiasis or endemic stone disease (Lu and Needham 1967).In Greece, Hippocrates had earlier recognized both renal and bladder stone and recommended diuretics and ingestion of large quantities of water for their removal. He considered wounds of the bladder wall as invariably fatal and therefore specifically forbade his followers to cut for the stone.
The Assyrian Book of Medicine, probably written around 300 B.C., includes much of the work of Hippocrates. Among the numerous prescriptions for various maladies are two elaborate potions for flushing out or dissolving renal stones. The latter recipe contains 50 substances with particular emphasis on camphor and vinegar. Other Assyrian works contain directions for infusing various preparations into the bladder through a bronze tube to dissolve bladder stones (Thompson 1934).
In Alexandria around 100 B.C., Ammonios developed an instrument for crushing stones within the bladder. In the first century A.D. in Alexandria, Rufus of Ephesus gave detailed instructions for removing bladder stones through a transverse perineal incision.
In Rome during the same century, Celsus performed numerous operations for bladder stone in boys 9 to 14 years of age. His eight-volume De Medicina contains a precise description of transverse perineal lithotomy followed almost without modification until the sixteenth century. Galen described the lateral perineal lithotomy, but, more importantly, noted the frequent occurrence of bladder stone in young boys. He also tried giving stone solvents (Iithotryptics) in an effort to dissolve the stones.
In Arabic medicine, Rhazes at about the turn of the tenth century described both renal and bladder stones, and he implicated increased salt intake and hot weather as factors in renal stone formation. Around a century later, Avicenna thought that bladder stones formed when the urine contained an excess of matter (Bitschai 1952).
By the eighteenth century, more and more sur-
Table VΠL154.2. Paleopathological specimens of renal and bladder stones
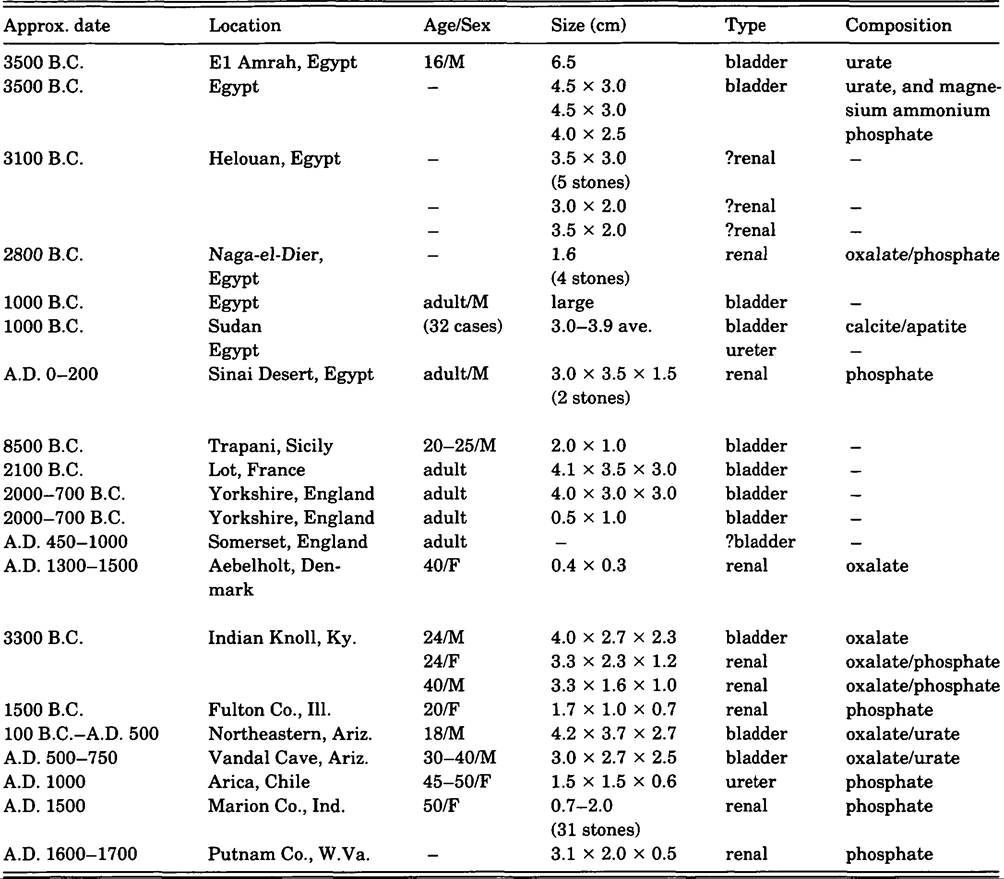
geons were attempting the dangerous lateral perineal lithotomy. Special hospitals for bladder stone patients were opened in England, France, Holland, and elsewhere. In 1753, Fri⅛re Come opened such a hospital in Paris and operated on over 1,000 patients. The Norfolk and Norwich Hospital was founded in 1771, and one of every 55 admissions in this endemic region was for removal of bladder stone.
Through paleopathology and careful archaeological technique, actual specimens of ancient renal and bladder stones have been recovered from skeletal and mummified remains. This material has been extensively reviewed elsewhere and is summarized in Table VIII. 154.2 (Steinbock 1985).
R. Ted Steinbock
Bibliography
Anderson, D. A. 1962. The nutritional significance of primary bladder stones. British Journal of Urology 34: 160-77.
1969. Historical and geographical differences in the pattern of incidence of urinary stones considered in relation to possible etiological factors. In Renal stone research symposium, ed. A. Hodgkinson and B. C. Nordin. London.
1972. Environmental factors in the etiology of urolithiasis. In Urinary calculi: International symposium on renal stone research, 130—44. Madrid.
Assendelft, E. 1900. Bericht uber 630 Stationar be- handelte Steinkranke. Archiv fiir Klinische Chirurgie 60: 669-80.
Batty Shaw, A. 1970. The Norwich School of lithotomy. Medical History 14: 221—59.
1979. East Anglian bladder stone. Journal of the Royal Society of Medicine 72: 222—8.
Bitschai, J. 1951. Calculosis of the urinary tract in Egypt. Journal of the Mount Sinai Hospital 17: 630—43.
1952. The history of urology in Egypt. American Journal OfSurgery 83: 215—24.
Brown, R. K., and E. C. Brown. 1941. Urinary stones: A study of their etiology in small children in Syria. Surgery 9: 415—24.
Eckstein, H. B. 1961. Endemic urinary Iithiasis in Turkish children. Archives of Disease in Children 36: 137-45.
Ellis, H. 1970. A history of bladder stone. Oxford.
Halstead, S. B. 1961. Bladder stone in Thailand: A review of the problem. American Journal of Tropical Medicine and Hygiene 10: 918—25.
Halstead, S. B., and A. Valyasevi. 1967. Studies Ofbladder stone disease in Thailand: Epidemiologic studies in Ubol province. American Journal of Clinical Nutrition 20: 1329-39.
Halstead, S. B., A. Valyasevi, and P. Umpoaivit. 1967. Studies of bladder stone disease in Thailand: Dietary habits and disease prevalence. American Journal of Clinical Nutrition 20: 1352—61.
Heyadat, S., and P. Amirshahy 1970. Urinary Iithiasis in Iran. Tropical and Geographical Medicine 22: 416—22.
Lonsdale, K. 1968. Human stones. Science 159:1199-207. Lonsdale, K., and P. Mason. 1966. Uric acid, uric acid dihydrate, and urates in urinary calculi, ancient and modern. Science 152: 1511-12.
Loutfi, A., R. van Reen, and G. Abdel-Hamid. 1974. Studies on bladder stone disease in Egyptian children. Journal of the Egyptian Medical Association 57: 96—114.
Lu, G. D., and J. Needham. 1967. Records of diseases in ancient China. In Diseases in antiquity, ed. D. R. Brothwell and A. T. Sandison, 222-37. Springfield, Ill.
Madden, F. C. 1913. The incidence of stone in Egypt. Lancet 2: 132—5.
McCarrison, R. 1931. The causation of stone in India. British Medical Journal i: 1009—14.
Modlin, M. 1967. The etiology of renal stone. Annals of the Royal College of Surgeons 40: 155-78.
Prien, E. L. 1971. The riddle of urinary stone disease. Journal of the American Medical Association 216: 503-7.
Racic, J. 1935. Calculus of the bladder in Dalmatia. Urologic and Cutaneous Review 39: 158-63.
Robertson, W. G. 1978. Risk factors in calcium stone disease of the upper urinary tract. British Journal of Urology 50: 449—54.
Robertson, W. G., et al. 1979. The effect of high animal protein intake on the risk of calcium stone formation in the urinary tract. Clinical Science 52: 285—8.
Stark, H. 1970. Childhood urolithiasis in northern Israel. Israel Journal of Medical Science 6: 341-5.
Steinbock, R. T. 1985. The history, epidemiology, and paleopathology of kidney and bladder stone disease. In Health and disease in the prehistoric southwest, ed. C. F. Merbs and R. J. Miller, 177-209. Tempe, Ariz.
Thomas, J. M. R. 1949. Vesical calculus in Norfolk. British Journal of Urology 21: 20—3.
Thompson, R. C. 1934. Assyrian prescriptions for diseases of urine. Babyloniaca 14: 96-120.
Thomson, J. O. 1921. Urinary calculi at Canton Hospital, China. Surgery 32: 44-56.
Valyasevi1 A., and A. Dhanamitta. 1968. Current research on pediatric bladder stone disease in Thailand. Journal OfVitaminology 14: 40—7.
More on the topic 154 Urolithiasis (Renal and Urinary Bladder Stone Disease):
- 154 Urolithiasis (Renal and Urinary Bladder Stone Disease)
- Contents
- Kiple Kenneth F. (Editor). The Cambridge World History of Human Disease. Cambridge University Press,1993. — 1200 p., 1993