Coronary Disease
Coronary disease has become the major form of heart disease in industrialized countries. As such, it has become a major object of attention for health care workers. Much of that attention has been focused on explaining the geographic and historical changes in the pattern of disease.
Heart disease caused 979,000 deaths in the United States in 1986. Accounting for 47 percent of all deaths, it is by far the leading cause of death, with myocardial infarction the most common diagnosis. Many more people suffer from heart disease than die from it. In the United States, there were an estimated 57,700,000 people with cardiovascular disease in 1983, 21,500,000 of whom had heart disease and 7,200,000 of whom had coronary heart disease. Of those with heart disease, 12,600,000 were under age 65, as were 3,200,000 of those with coronary heart disease. The physical activity of one-quarter of those with heart disease was limited, making the condition an important cause of disability as well as death.
Declining Coronary Death Rate in the United States
At the turn of the nineteenth century, heart disease was the fourth leading cause of death in the United States, behind pneumonia and influenza (combined), tuberculosis, diarrhea, enteritis, and ulceration of the intestines. All of these produced death rates in excess of 100 per 100,000 population. A sharp upward trend in coronary disease became apparent around 1920, and coronary disease was recognized with increasing frequency throughout most of the first 50 years of the twentieth century. By 1940 only two disease categories with death rates of more than 100 per 100,000 remained: cancer and diseases of the heart. The death rate from heart diseases then began a dramatic series of changes.
As Figure ∏.5.1 shows, the death rate reached a peak in 1963 and has declined continuously since then.
There was some initial concern about whether the decline was real or only a product of a 1968 change in disease classification. But now there is little doubt that the death rate for coronary heart disease in the United States has fallen dramatically since the 1960s. However, that decline has not been evenly distributed. The mortality rate for heart diseases in California, for example, peaked relatively early, around 1955, and the subsequent decline there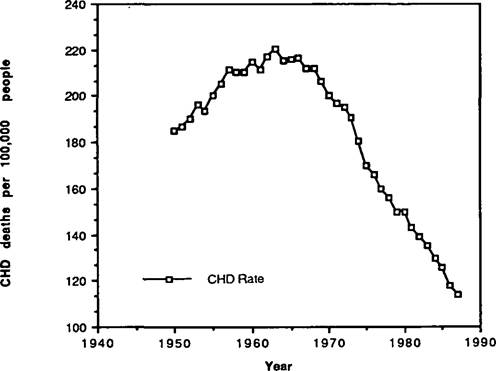
Figure II.5.1. Rate of coronary heart disease per 100,000 people in the United States (age-adjusted to 1940 age distribution). (Data from Vital Statistics of the United States, as prepared by the National Heart, Lung, and Blood Institute; data for 1987 provisional.)
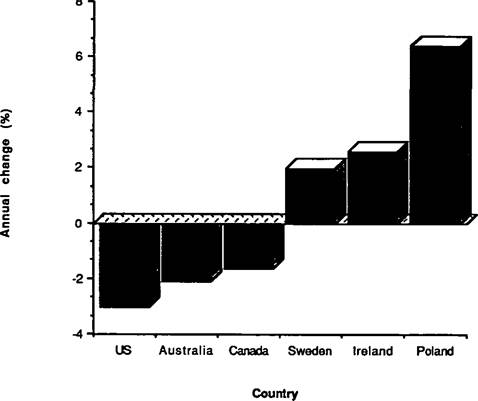
Figure II.5.2. Annual change in mortality from ischemic cardiac disease, 1968-77 (men aged 40 to 69). (Data from WHO MONICA 1988.)
was repeated in other parts of the United States throughout the 1960s and 1970s. By 1986 the death rate for coronary heart disease was 55 percent of the 1966 rate, and the decline in the death rate for all cerebrovascular diseases was proceeding three times faster than the decline for all other causes of death combined.
Worldwide Variation in CoronaryDiseases
Such countries as Australia, New Zealand, and Canada have experienced similar declines in the death rate from coronary disease among men. Other countries, however, have experienced significant increases in death rates, as revealed in Figure II.5.2. These have included countries, such as Scotland and Northern Ireland, with death rates initially comparable to that of the United States, as well as countries, such as Poland and Switzerland, initially having death rates much lower than that of the United States.
Some of the increase may be due to the impact of industrialization.
In China, for example, infectious diseases such as tuberculosis and nutritional deficiencies were the major causes of morbidity and mortality, with cardiovascular disease of little concern until the late 1950s. Even among industrialized countries, the rate of death from cardiovascular diseases has varied widely, from 913 per 100,000 in Finland (for men aged 40 to 69 in 1975) to 379 in Japan.Attempts have been made to explain these differences in disease rate. The World Health Organization’s Multinational Trends and Determinants in Cardiovascular Disease (MONICA) has made one such attempt. With 41 projects in 21 countries, MONICA is helping to make cardiovascular disease a focus of international and cross-cultural comparisons. Only AIDS has received similar worldwide attention.
Studies of changing patterns of cardiac disease have contributed to the invention of risk factor, a concept that is receiving widespread attention as a way of conceptualizing the cause of many diseases. Unlike infectious diseases, which are defined in terms of a single, specific agent, risk factor is conceptualized on an epidemiological and probabilistic basis.
Risk Factors for Coronary Heart Disease
Much of our current explanation for the historical and geographic differences in death rates from coronary heart disease derives from the concept of risk factor. A number of long-term prospective studies have enhanced the utility of this concept. The most widely known study is the Framingham Heart Study, in which 5,209 men and women have been carefully examined every two years since the investigation began in 1948 in Framingham, Massachusetts. Studies such as this have identified a number of factors that contribute to the likelihood of developing coronary heart disease. Some of these cannot be modified. For example, men are more likely to suffer from heart disease than women; older people are more likely to develop the disease than younger ones; and those having a family history of early cardiac disease are at greater risk than those without such a history.
However, other factors can be modified. Cigarette smoking dramatically increases the likelihood of a coronary event and represents the greatest and most preventable cause of heart disease. Once a person stops smoking, the risk rapidly declines to a level approximately the same as it would be if the person had never smoked. High blood pressure and diabetes are also important risk factors.
A positive relationship between blood cholesterol level and the development of heart disease has been clearly demonstrated. Almost no Japanese men have serum cholesterol levels above 200 mg∕dl, whereas almost no Finnish men have concentrations below that level. Consistent with the hypothesis that cholesterol is associated with death from coronary heart disease, the death rate from coronary heart disease in Finland is more than 10 times that in Japan. Historical analysis has shown that the death rate from heart disease in Europe fell during the Second World War, presumably as a result of a lack of foods that elevate serum cholesterol level. Most population-based studies have shown a consistently positive relationship between increased serum cholesterol level in the form of low-density lipoprotein and the rate of heart disease. At high levels the association is particularly strong; the risk of death for persons having cholesterol values in the top 10 percent is four times the risk of persons in the bottom 10 percent. There is now good evidence that lowering cholesterol level with drug therapy will lower the death rate from coronary disease. This effect of reducing cholesterol level is most beneficial for those having the highest levels, but the value of reducing cholesterol level for those without elevated cholesterol remains unclear.
Exercise has a beneficial effect on the types of lipids circulating in the bloodstream. Although obesity is associated with hypertension, whether obesity is an independent risk factor for coronary heart disease is as yet unclear.
In the 1950s some U.S.
investigators argued that people who were hard-driving, competitive, overcommitted, impatient perfectionists and who found it difficult to relax-these with the so-called type A personality - were at increased risk for coronary heart disease. These findings have been a subject of intense debate. Some studies of workers in Great Britain have identified civil service manual workers, not those with the hard-driving behavior indicated in the original research, as those at greatest risk from their behavior type. Although the exact role of type A behavior as an independent risk factor in the development of coronary heart disease remains unclear, recent studies suggest that the type A personality may actually improve longevity after a myocardial infarction.Alcohol intake in small quantities - two or fewer drinks per day - may diminish the risk of developing coronary disease. However, alcohol in greater amounts is clearly associated with greater morbidity and mortality from both cardiac and noncardiac disease.
Explaining Change
Many investigators have attempted to use the concept of risk factor to explain geographic and historical changes in the rate of death from coronary heart disease. The decline in the U.S. death rate may have been due partly to improved medical interventions, including the widespread establishment of coronary care units, improvements in prehospital resuscitation and care, better surgical and medical treatment of those with known heart disease, and more extensive treatment of the large proportion of the population with hypertension. The decline may also have been due in part to changes in life-style. Cholesterol consumption peaked in 1959, and the percentage of North Americans who smoke has declined steadily over the past few decades. However, a significant part of the change cannot be fully explained.
Although coronary heart disease appears to be an increasing cause of death in developing countries, accounting for 15 to 25 percent of all deaths as the mean life expectancy reaches 50 to 60 years, more is required to explain the rates of death from coronary heart disease than merely to blame increasing industrialization.
People moving from one industrialized country to another tend to develop the susceptibility to heart disease prevalent in the host country, suggesting that other environmental factors play an important role in determining the incidence of heart disease. Striking confirmation of this comes from a study of 11,900 people OfJapanese ancestry living in Japan, Hawaii, and California. Those living in Japan had the lowest incidence of heart disease, those living in Hawaii had an intermediate incidence, and those living in California the highest. The best predictor of the incidence of heart disease among those living in California was not the presence of known risk factors, but the extent to which those Japanese who had moved from Japan to California continued to adhere to traditional Japanese values: those who retained more of these values had a lower rate of heart disease.