62 Gonorrhea
The name gonorrhea, which means “flow of seed,” and its vernacular counterparts (“clap,” “dose,” “strain”), reflect a hazy comprehension of the disease. The only accurate term in common use is “drip,” which acknowledges the white-to-yellowish milky discharge from the male penis.
But even this more honest description includes only the male urethral portion of a broader syndrome.Gonorrhea is an infection of mucosal surfaces caused by a small gram-negative bacterium - the gonococcus — whose only reservior in nature is human. Its presence in the lower male or female genital tract defines the condition gonorrhea; otherwise, the adjective “gonococcal” is used to precede a generic infective syndrome (as in “gonococcal endocarditis”). Though gonorrhea is transmitted primarily to genital mucosa through sexual contact, it may cause localized abscesses or generalized dissemination, with infection of the skin, heart valves, joints, and central nervous system. It is rarely the cause of death, but, if untreated, it produces serious sequelae in both men and women.
The gonococcus, Neisseria gonorrhoeae, shares an ecological niche with other sexually transmitted pathogens such as Chlamydia trachomatis, Urea- plasma ureslyticum, and T-mycoplasmas. It depends for its survival on variable virulence, sufficient numbers of asymptomatic infectees, an ability to produce a rapid genomic response to antibiotic pressure, a symbiotic relationship with new pieces of genetic material (called plasmids), and propitious set of social and sexual mores among its hosts. As history demonstrates, this seemingly delicate balance has been universally available.
Etiology and Diagnosis
The causative agent of gonorrhea is the gonococcus (N. gonorrhoeae) - a small, diplococcus whose flattened apposing surfaces, tinctorial properties (when stained by Gram’s method), and association with polymorphonuclear leukocytes provide a typical microscopic picture.
In certain sites (e.g., urethra, joint, cerebrospinal fluid, ocular conjunctiva), demonstration of the typical morphology is virtually diagnostic. From other sites (rectum, pharynx), however, the possible presence of other gonorrhea types renders the Gram-stained smear less sensitive. For all sites, culture of the organism on artificial media is required for diagnostic assurance. Confirmation requires typical morphology, demonstration of indophenol oxidase production, and the ability of the organism to metabolize glucose, but not fructose, maltose, sucrose, or mannitol.Clinical Manifestations
Genital Site Infections in Men and Women
Pus issuing from the penile opening, often accompanied by discomfort, pain, or burning on urination, is the most frequently recognized clinical manifestation of gonorrhea. The gonococcus adheres to cells that line the distal urethra, establishing - in the symptomatic individual - an inflammatory reaction and the subsequent outpouring of polymorphonuclear leukocytes. (This primary pathological process is basically the same at all mucosal sites of infection.) Though the majority of men will become symptomatic 3 to 5 days after adequate exposure, the clinical spectrum varies. In perhaps one-quarter of patients, pain or discharge will be attenuated or Subsymptomatic (i.e., insufficient to cause the patient to seek medical care). In addition, a substantial proportion of men with gonorrhea will be asymptomatic. Before the advent of antibiotics, the major sequelae of male urethral infection were postinflam- matory fibrosis and stricture of the urethra. Such complications are now rare.
Though women have long been known to harbor the organism, only recently have distinct clinical syndromes been identified. Part of the delay is due to the fact that asymptomatic infection probably occurs more frequently in women, and little clinical attention is paid to the “normal” vaginal discharge. Infection of the female urethra occurs in 70 to 90 percent of women with gonorrhea, but rarely in the absence of concomitant infection of the endocervix.
The more important lower tract manifestation of gonorrhea in women is infection of the uterine cervix. A syndrome of purulent or mucopurulent endocervical discharge characterizes the infection. Though the clinical diagnosis may be complicated by the coexistence of infection with other pathogenic organisms, cervical mucopus is clearly not “normal” and requires systematic bacteriologic investigation.Both sexes contract anal and throat infection from direct exposure to infected penile secretions. Both are associated with symptoms in a minority of cases. Asymptomatic rectal infection probably plays a major role in transmission. Throat infection is of minor importance, except as a site for dissemination of the gonococcus into the bloodstream.
Pelvic Inflammatory Disease (PID)
Perhaps the major modern concern about gonorrhea is its potential for destruction of female reproductive organs. The gonococcus may spread upward from the cervix to inflame the uterine lining of the fallopian tubes (salpingitis) and ultimately cause peritonitis. Once established, PID becomes chronic, of long duration, and with serious consequences. Approximately 20 percent of women will have a recurrence after treatment for a primary episode of gonococcal PID. The syndrome of chronic pain, lower abdominal discomfort, and dyspareunia reflects insidious scarring and closure of the fallopian tubes, which may cause ectopic pregnancy and lead ultimately to involuntary infertility. Studies in Sweden indicate that the risk of sterility is 12 to 16 percent after a single episode of salpingitis and rises to 60 percent after three episodes.
Disseminated Gonococcal Infection (DGI)
An uncommon but distinctive picture appears when the gonococcus is spread via the bloodstream. The classic picture includes (often) asymptomatic infection of the pharynx, penis, vagina, or rectum in association with characteristic skin lesions and arthritis. The skin lesions are small, hemorrhagic areas with necrotic centers, and generally number fewer than 20.
The infected joint(s) usually exhib- it(s) the four classic features of arthritis: swelling, redness, pain, and heat. The knee is most frequently involved, followed by elbows, ankles, wrists, and small joints of the hand. Patients with DGI usually respond well to routine treatment and rarely suffer long-term musculoskeletal complications.Other Clinical Manifestations
A variety of other rare infections with the gonococcus have been documented. Adults occasionally develop gonococcal conjunctivitis, with a potential for more serious ocular involvement, through direct (i.e., hand-to-eye) contact with infected secretions. Gonococcal endocarditis, myocarditis, hepatitis, and meningitis may occur as part of the disseminated syndrome. Perihepatitis (termed the Fitz-Hugh- Curtis syndrome) has traditionally been attributed to gonococcal infection in the upper right quadrant, usually in association with classic PID. Recent evidence, however, indicates that the syndrome is more often associated with chlamydial, rather than gonococcal, infection.
Gonococcal Infection in Children
The other major mode of transmission of the gonococcus is from mother to child. A newborn may become infected during passage through an infected birth canal, and the most common clinical manifestation is gonococcal ophthalmia. The typical syndrome includes the development of purulent discharge from one or both eyes with relatively rapid progression, in the untreated child, to more generalized ocular involvement, scarring, and blindness. The use of routine eye prophylaxis with silver nitrate (see discussion under History, below) was a landmark in preventive medicine and greatly reduced the occurrence of this syndrome. Children may develop gonorrhea in sexual sites as well. It has become apparent, in recent years, that the majority of infected children have suffered sexual abuse. In boys, symptomatic or asymptomatic anogenital infection may occur. In girls, the primary manifestation is a vulvitis, because the prepubertal cervix is not an adequate milieu for survival of the gonococcus.
Classification, Immunology, and Pathology The importance of gonorrhea is measured not only by its considerable burden of acute disease and longterm consequences, but also by some of its extraordinary biological characteristics. The virulence of the gonococcus rests in its ability to adhere to muscosal surfaces, to resist immunological defenses, to cause asymptomatic infection, and to resist antibiotic killing. These qualities have been important in the development of four major classification schemes based upon the following:
1. The presence or absence of pili (long, filamentous projections on the surface of the gonococcus), which determine adherence to mucosal cells. Their presence is, in turn, reflected in the size, shape, and opacity of gonococcal bacterial colonies, and forms the basis for the earliest classification scheme used.
2. The nutritional requirements of the gonococci. Typing of organisms based on their need for certain amino acids (auxotyping) has determined the presence of special strains that are more or less sensitive to antiobiotics, and that have a greater propensity to cause disseminated infection.
3. The antigenic structure of the gonococcal cell envelope, which provides a mechanism for classification (serovars). Serovars have been used, in conjunction with auxotyping, to show patterns of distribution and to link cases epidemiologically.
4. Susceptibility to antibiotics. Four transferable pieces of genetic material (plasmids) have been identified, which have helped in geographic localization of cases.
These systems for classification reflect the considerable pathogenetic repertoire available to the gonococcus. In contrast, the immunologic armamentarium of the host seems inadequate. Genital secretions may have some inhibitory effect on gonococci in vitro, but are not protective. Local immunoglobulin production has been demonstrated but may be counteracted by protease produced by the gonococcus. Serum antibody is usually demonstrable in previously infected persons, but resistance to serum killing is a typical feature of freshly isolated gonococci.
Indeed the net result of studies to date simply reflects the time- honored observation that people may contract gonorrhea again and again. There is no apparent protective human immunity. The existence of asymptomatic infection, and the apparent immunologic tolerance of the host, may account in part for the ecological success of the gonococcus.Distribution and Incidence
Gonorrhea is found worldwide, but documentation of its true extent is lacking. Direct comparisons of incidence among nations are difficult to make because of the wide variation in clinical and diagnostic facilities, the extent of disease reporting, and the degree of care given to case finding. The disease is widespread in both the industrialized and the developing world, but it is likely that the burden on developing nations is greater. It is estimated that the incidence in some large African cities may be as high as 3,000 to 10,000 per 100,000 population. Because gonorrhea is, in principle, a disease of high incidence and low prevalence, it is noteworthy that surveys of women attending prenatal and family planning clinics in Africa disclose a prevalence as high as 17 percent. Among prostitutes in Latin America, Asia, and Africa, the prevalence of gonorrhea may be 30 to 50 percent. These are, of course, occasional surveys of selected populations, but, in the absence of systematic information, they provide some sense of the magnitude of the problem.
A number of industrialized nations, on the other hand, do have systematic reporting of gonorrhea. Routinely collected statistics have permitted documentation of the major epidemiological event in the history of gonorrhea: a worldwide pandemic that began in the late 1950s and peaked in the mid-1970s.
A comparison of disease rates in the United States, the United Kingdom, Sweden, and Canada (Figure VIII.62.1), all of which have advanced
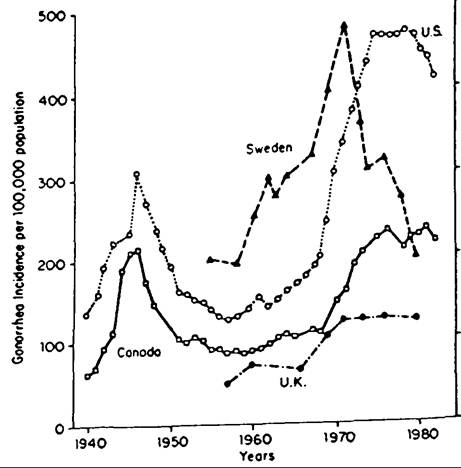
Figure VIII.62.1. Gonorrhea incidence in selected countries, 1940—83. (From R. C. Bames and K. K. Holmes.
1984. Epidemiology of gonorrhea: Current perspectives. Epidemiological Reviews 6: 1-30; 3, fig. 1, by courtesy of Epidemiological Reviews and the American Journal of Epidemiology.)
health care systems, indicates a rise in gonorrhea occurrences ειfter World War ∏, with a subsequent fall to a nadir in the mid-1950s. Though varying in size and timing, an increase in gonorrhea throughout the 1960s, with termination of the accelerated rise by the mid-1970s, was experienced by each nation. The graph is representative of the situation for most industrialized countries during the interval, and conveys the disparity with which nations were apparently affected. At the peak, in the mid-1970s, rates among industrialized nations differed by as much as 10-fold. (By contrast, rates among developing nations during the interval differed even more wildly, but here the variation in reporting clearly plays an important role.)
The impact and specific features of the pandemic may be demonstrated by examining the history of the disease in the United States during this period. Between 1956 and 1985, rates of gonorrhea increased in all age groups for both men and women (Figure VIII.62.2). Rates for females are higher at younger ages, and peak at ages 15 to 19 years. Rates for males peak at ages 20 to 24, producing a crossover pattern (Figure VIII.62.3). The origin of this increase, and of the pandemic in general, is not fully understood. It is often attributed to changes in sexual mores during the 1960s and 1970s, with major increases reported in the frequency of premarital sexual experiences by both men and women, a greater availability of contraceptive technology, and an increase in the number of individuals entering the age of sexual activity (the so-called baby boom generation).
It is likely that the pandemic has not yet had its full impact on the developing world, though the peak in industrialized nations seems to have passed. If so, the burden of morbidity, long-term sequelae, and mortality will continue to have a major influence on
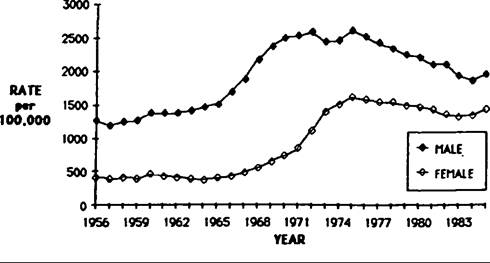
Figure VΠI.62.2. Gonorrhea rates in men and women, aged 20-4, United States, 1956-85.
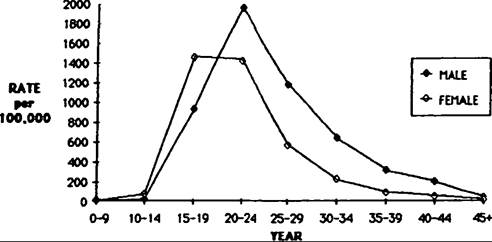
Figure VIII.62.3. Gonorrhea: age-specific rates for men and women, United States, 1985.
80 percent of the world’s population in the coming years.
History
Gonorrhea is the oldest, as well as the most common, of the venereal diseases. An Egyptian papyrus from approximately 3500 B.C. prescribes plant extracts to soothe painful urination. The Hebrew Bible makes reference to treatment of genital exudates, which may well refer to gonorrhea. Hippocrates recognized the venereal nature of transmission at about the beginning of the fourth century B.C., and Galen, in the second century A.D., is believed to have coined the name. In the fourteenth century, a description of the ailment that stressed a major symptom, chaude pisse, or “hot piss,” led to the disease’s receiving this appellation from the French.
By 1500 or so, interest centered on the distinction between syphilis and gonorrhea. The majority opinion appeared to favor the notion that they were different manifestations of the same disease, particularly because syphilis was so clearly protean in its manifestations. However, in the middle of the sixteenth century, a French physician, Jean Femel, wrote of gonorrhea as a separate disease from syphilis in his Medicina. The British physician Francis Balfour, writing two centuries later, has also been credited with the belief that syphilis and gonorrhea were distinct.
Confusion set in, however, following John Hunter’s argument that the cause of both diseases was the same and that gonorrhea was a manifestation of the disease on a secreting surface (mucosa) whereas syphilis was its manifestation on a nonsecreting surface (skin). To prove this, he infected himself with pustular discharge from a patient he thought had gonorrhea, and developed syphilis instead. The patient may have been dually infected, but at any rate, this was an unfortunate instance of a brilliant and heroic use of the scientific method gone wrong, and it postponed scientific understanding of the two diseases for decades.
It was during this same period (1760-90) that the most lucid literary account of gonorrhea appeared. James Boswell, the biographer of Samuel Johnson, kept a meticulous diary of his own repeated encounters with gonorrhea. The diary details the clinical manifestations and psychological effects of 19 episodes. There is little question of the impact of gonorrhea on his life, and, by extension, on the life of countless others in the era. He is believed to have died of gonorrheal complications.
In the 1790s, Benjamin Bell of Edinburgh, who was in disagreement with Hunter, published several tracts that explored the clinical and epidemiological evidence for gonorrhea and syphilis as separate disease entities. He posed a number of simple questions: Why is gonorrhea more common when the skin of the penis is at greater risk of exposure than the urethra? Why are there geographic differences in the distribution of the two diseases? Why have their manifestations appeared in the same populations at different points in time?
It remained, however, for Philippe Ricord, in a series of clinical observations and direct experiments in the mid-1800s, to provide a definitive distinction between the two diseases. It is of interest that Ricord commented that there is no justification for experimentation with grave diseases in human beings, although he inoculated 17 prisoners with gonorrheal pus, producing occasional ulcers with prompt healing, but no evidence of syphilis.
In 1879, Albert Neisser, an assistant in dermatology at the University of Breslau, Germany, published his preliminary findings which confirmed the conclusions of Ricord by describing the organism that now bears his name. This was probably the second description of a major human pathogen (after Koch’s identification of the anthrax bacillus 3 years earlier). In 1882, the organism was first grown in vitro by Ernst von Bumm. The first major preventive action was taken in the following year when Karl Siegmund Crede, at the Lying-In Hospital in Leipsig, recognized the benefit of instillation of 2 percent silver nitrate solution (later reduced to 1 percent) in the eyes of newborns. The occurrence of gonococcal ophthalmia diminished rapidly with the widespread adoption of this procedure.
Unfortunately, advances did not follow in rapid succession. In fact, after the initial diagnostic procedures were established, there were no major improvements in the understanding of gonorrhea until the sulfonamides (e.g., sulfamidochrysoidine, Prontosil) were introduced in 1937. This success was shortlived, and true antibiosis for gonorrhea appeared only in the 1950s with the general availability of penicillin. The next critical breakthroughs were the description of the different colonial morphologies by Douglas S. Kellogg et al. in 1963 and the development of a selective medium for culturing the gonococcus by James D. Thayer and John E. Martin in 1964. Subsequent events, including the worldwide pandemic of the 1960s and 1970s, and the major advances in immunology and molecular biology, were alluded to earlier. Clearly, it is only in recent times that gonorrhea’s effect on us, and in turn, our ability to alter its course, have dramatically changed.
Geography
Through gonorrhea is found worldwide, the lack of systematic data precludes meaningful global mapping. But even if national rates were universally available, a local approach might be more informative. In its transmission, its endemicity, and its continued propagation, gonorrhea is a neighborhood disease. An understanding of the local geography is predicated on a coherent theory for transmission.
Epidemiology
The clinical epidemiology of the classic gonorrhea syndromes forms the basis for the population epidemiology of the disease. Gonorrhea is transmitted by sexual contact. The probability of transmission from male to female after a single contact is approximately 50 percent; from female to male, 22 percent. The incubation period is 3 to 5 days in men and slightly longer in women. A significant proportion of both sexes never becomes symptomatic. The incidence of disease in a given community, then, is a function of two major parameters: (1) the degree of sexual interaction, which includes the frequency of new partners, as well as the duration, intensity, frequency, and logistics of sexual contact; and (2) the duration of infectiousness, which takes into account the proportion of asymptomatic infection, the proportion of a population that will seek health care, the adequacy of therapy, and the extent to which sex partners are apprised of their risk. Clearly, the final epidemiological picture will be a complex interaction of biological, social, and individual events. In general, however, gonorrhea is a disease of high incidence but short duration and, hence, of low prevalence.
Transmission Dynamics
Beginning in the early 1970s, mathematicians Herbert Hethcote and James Yorke constructed a theoretical framework for the transmission dynamics of gonorrhea. Using some of the concepts of population ecology, they noted that the reproduction rate for gonorrhea (i.e., the ability of an infected person to replace him- or herself) must be determined when the disease is at endemic equilibrium. In the steady state, therefore, each infected person must have two “adequate” contacts for transmission on average (“adequate” means that the gonococcus is transmitted). There must be a “source” contact and a “spread” contact for disease propagation. Because not all sexual contacts are “adequate,” it follows that the average number of total contacts must be greater than 2.
In constructing a model of transmission dynamics, several key epidemiological observations must be considered:
1. Gonococcal infection does not confer protective immunity; thus an individual is “immune” only when infected.
2. Individuals become infectious soon after exposure; there is, then, no “exposed, incubating” group to be considered in a model.
3. Seasonal variation of gonorrhea is well defined, with a peak in late summer in temperate climates, but the variation is small (about 10 percent) in comparison with other diseases. This implies that the parameters used in the model can be constant.
4. Data derived from interviewing gonorrhea patients about their sex partners suggest that the average number of “adequate” contacts is well below 2. In 1985, there were only 0.3 infected contacts found for each person with gonorrhea interviewed. Even with allowances for slippage in the system of interviewing cases, finding contacts, and bringing them to medical examination, this is far below the two infected contacts per case needed to maintain a reproduction rate of 1 and to preserve endemic equilibrium.
It was reasoned, then, that the observed number of infected contacts per case is a weight average of two groups: (1) those for whom one or no contacts were identified (nontransmitters); (2) those with two or more contacts identified (transmitters). Those in the first group - the vast majority of gonorrhea infectees - were unlikely to pass the infection to another person. Hethcote and Yorke hypothesized that the transmitters - those who actually maintain the endemicity of gonorrhea - were drawn from so-called core groups. These groups were defined as persons with stable sociodemographic and geographic characteristics who constituted a small minority of cases (under 5 percent), but who accounted - either directly or indirectly - for most gonorrhea transmission. It is within such groups that the epidemiological features of gonorrhea (no immunity, immediate infectiousness, year-round transmission) were fully operative. The limit to gonorrhea spread within a core group was termed the saturation effect: that is, sexual contact between infected persons.
In a series of elegant mathematical discussions, Hethcote and Yorke developed a model for the dynamics of transmission based on population compartments that included core and noncore groups. They were able to demonstrate the plausibility of an equilibrium state in which most cases were attributable to small groups of active transmitters. Parallel with this theoretical development, some empirical evidence for the physical existence of core geographic areas and definable core groups emerged.
It was shown in 1979, based on the routine reporting of gonorrhea morbidity data, that the city of Denver contained four different areas with high concentrations of infectees (see Figure VIII.62.4). Each geographic area housed a distinct population subgroup: black heterosexuals, Hispanic heterosexuals, white homosexual men, and military recruits.
Through analysis of over 120,000 geocoded cases
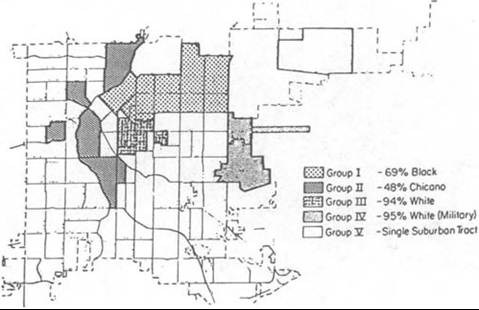
Figure VΠI.62.4. Distribution of gonorrhea in Denver, Colorado, 1974-6. [From R. B. Rothenberg. 1979. Analysis of routine data describing morbidity from gonorrhea.
Sexually Transmitted Diseases 6(1): 5-9; 6, fig. 1, by courtesy of LippincottZHarper & Row, Philadelphia, Penna.]
of gonorrhea in upstate New York from 1975 to 1980, a general geographic pattern emerged. Within all 12 Standard Metropolitan Statistical Areas (SMSAs, the urban centers), there was intense concentration of gonorrhea in a small number of contiguous census tracts (core areas) within the inner cities. In a concentric circle surrounding the core were a group of census tracts with somewhat lessened gonorrhea rates (adjacent areas). The rest of the SMSA constitutes the peripheral area, with a markedly diminished gonorrhea burden. The concentration of gonorrhea in the core area was 20-fold higher than that for New York State in general, and several of the census tracts in the core had rates that were 40-fold higher. Not only was this pattern repeated in all SMSAs, but all the core areas were similarly characterized by high population density and low socioeconomic status. The geographic configuration for Buffalo, New York, is typical (Figure VIII.62.5).
This pattern was also documented in Colorado Springs, Colorado, using data collected from inter
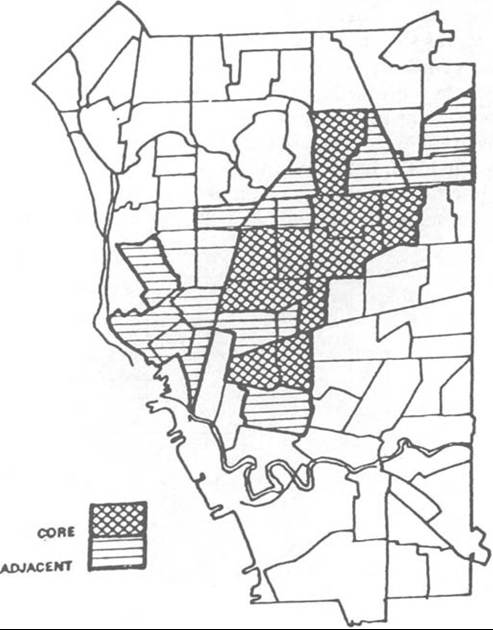
Figure VΠI.62.5. Occurrence of gonorrhea in Buffalo, New York, 1975—80; distribution of core and adjacent tracts. (From R. B. Rothenberg. 1983. The geography of gonorrhea: Empirical demonstration of core group transmission. American Journal OfEpidemiology 117(6): 688— 94; 691, fig. 1.)
views of 97 percent of the cases that occurred during a 6-month interval. Again, clustering of over 50 percent of the cases was demonstrated in about 5 percent of census tracts. Social aggregation of cases was demonstrated by the consistent use of six drinking establishments by a major proportion of infectees, and by the aggregation of patients and their sexual partners in the same census tracts. Contrary to commonly held belief, the majority of sexual partners had known each other socially prior to sexual contact. The interconnection of individuals in networks could be demonstrated through linkage provided by the interview process. Further analysis demonstrated that the core groups in Colorado Springs generated a high force of infectivity (i.e., days of potential transmission in infected exposed partners),
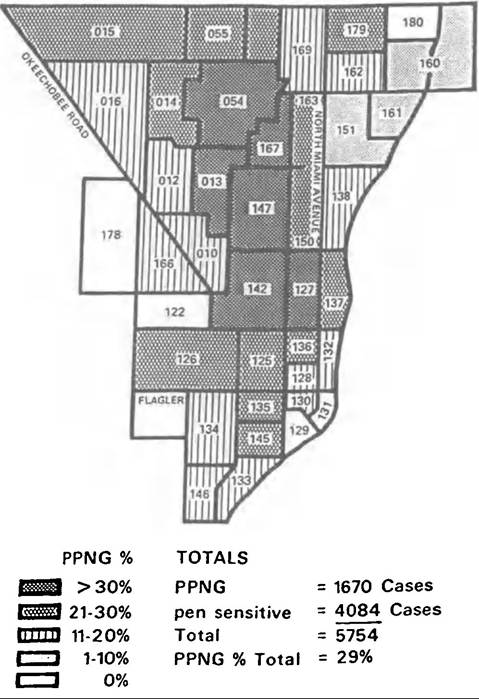
Figure VΠI.62.6. Penicillinase-producing Neisseria gonorrhea (PPNG) as percentage of total gonorrhea, by zip code analysis in Miami, Florida, March 1985 to February 1986. (From J. M. Zenilman et al. 1988. Penicillinaseproducing Neisseria gonorrhoeae in Dade County, Florida: Evidence of core-group transmitters and the impact of illicit antibiotics. Sexually Transmitted Diseases 15: 45-50; 47, fig. 2, by courtesy of LippincottZHarper & Row, Philadelphia, Penna.)
and had a heightened degree of sexual interaction both inside and outside their core groups.
Similar geographic clustering was documented in Seville, Spain, where it was noted that all the STD syndromes appeared to exhibit a similar geographic pattern. The presence of penicillin-resistant N. gonorrhoeae has provided a convenient marker for the demonstration of core-group aggregation as well. In an initial outbreak reported from Liverpool in 1976, clustering of cases occurred within two small inner- city districts. In Miami, a major endemic area for resistant gonorrhea in the United States, the clustering of resistant cases within presumed core-group areas paralleled that for all of gonorrhea (Figure VIII.62.6).
It cannot be assumed that the geographic characteristics displayed in these examples are universal. In particular, differences in human ecology and sexuality in developing countries may dictate a different pattern, and data are not yet available. It might tentatively be concluded, however, that a concentric pattern of gonorrhea risk, which diminishes outward from the central inner city, exists in many major ιu*ban areas. The potential for use of geographic patterns in the development of disease control strategies, and in the understanding of other sexually transmitted syndromes, is an area for further development.
Richard B. Rothenberg
This chapter was written in the author’s private capacity. No official support or endorsement by the Centers for Disease Control is intended or should be inferred.
Bibliography
Alvarez-Dardet, C., S. Marquez, and D. J. Peres. 1985. Urban clusters of sexually transmitted disease in the city of Seville, Spain. Sexually Transmitted Diseases 12(3): 166-8.
Bames, R. C., and K. K. Holmes. 1984. Epidemiology of gonorrhea: Current perspectives. Epidemiologic Reviews 6: 1-30.
Britigan, B. E., M. S. Cohen, and P. F. Sparling. 1985. Gonococcal infection: A model of molecular pathogenesis. New England Journal of Medicine 312(26): 1683-94.
Hethcote, H. W., and J. A. Yorke. 1984. Gonorrhea transmission dynamics and control. Lecture Notes in Biomathematics. New York.
Holmes, K. K. (Chairman). 1986. WHO Expert Committee on Venereal Diseases and Treponematoses. Technical ReportSeries No. 736. Geneva.
Holmes, K. K., et al. 1984. Sexually transmitted diseases. New York.
Hook, E. Q., and K. K. Holmes. 1985. Gonococcal infections. Annals of Internal Medicine 102: 229—43.
Kampmeier, R. H. 1977. John Hunter - a man of conviction. Sexually Transmitted Diseases 4(3): 114—5.
1978. Identification of the gonococcus by Albert Neisser. Sexually Transmitted Diseases 5(2): 71—2.
1979. The early identification of several venereal infections. Sexually Transmitted Diseases 6(2): 79—81.
Kellogg, D. S., et al. 1963. Neisseria gonorrhoeae: I. Virulence genetically linked to clonal variations. Journal OfBacteriology 85:1274-9.
Ober, W. B. 1969. Boswell’s gonorrhea. Bulletin of the New York Academy OfMedicine 45(6): 587-636.
Potterat1 B. A., et al. 1985. Gonorrhea as a social disease. Sexually Transmitted Diseases 12(1): 25—32.
Rice, R. J., et al. 1987. Gonorrhea in the United States 1975-1984: Is the giant only sleeping? Sexually Transmitted Diseases 14(2): 83-7.
Rothenberg, R. B. 1979. Analysis of routine data describing morbidity from gonorrhea. Sexually Transmitted Diseases 6(1): 5—9.
1983. The geography of gonorrhea: Empirical demonstration of core group transmission. American Journal OfEpidemiology 117(6): 688—94.
Thayer, J. D., and J. E. Martin. 1964. A selective medium for the cultivation of Neisseria gonorrhoeae and Neisseria meningitidis. PublicHealthReport 79: 49—57.
Zenilman, J. M., et al. 1988. Penicillinase-producing Neisseria gonorrhoeae in Dade County, Florida: Evidence of core-group transmitters and the impact of illicit antibiotics. Sexually Transmitted Diseases 15: 45-50.