International Comparisons of Maternal Mortality
Few countries published vital statistics before the mid-nineteenth century. The exception was Sweden, where, as UlfHogberg (1985) has shown, the MMR fell from about 100 per 10,000 births in 1750 to about 50 in the mid-nineteenth century, followed by a rise to about 63 in the 1870s.
Work by R. Schofield (1986) suggests that the MMR in England probably fell from about 100 per 10,000 births during 170050 to around 80 during 1750-1800 and to between 50 and 60 in the first half of the nineteenth century. The MMR in Europe in the late eighteenth and early nineteenth centuries may have been about 100 deaths per 10,000 births, but this is speculative.Data on maternal deaths were not always included in early lists of causes of death, but they were usually included in vital statistics (with various degrees of reliability) from the 1850s in European countries, from about the 1880s in Australia and New Zealand, and from 1900 in the United States (except for the state of Massachusetts, where statistics on maternal mortality can be obtained from 1850).
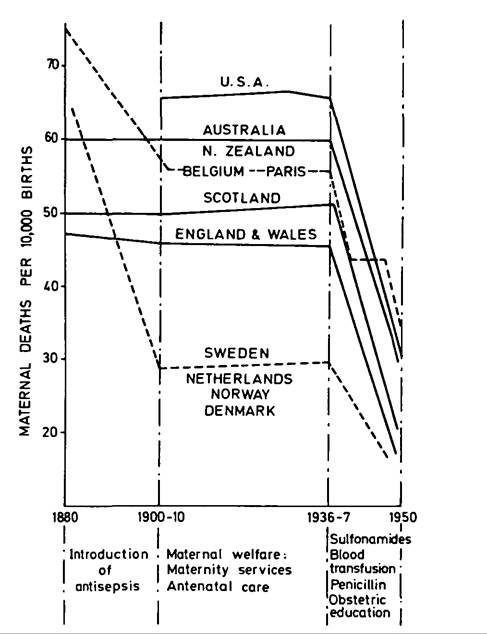
Figure ΓV.2.3. Changes in maternal mortality rates in different countries, 1880-1950. (Based on the vital statistics of the countries shown.)
Data from the United States as a unit present a special problem because they were based on the expanding Death Registration Area, established in 1880. Initially this consisted of the states of New Jersey and Massachusetts, the District of Columbia, and nineteen cities. Other states were added year by year. The process was completed by 1933 with those states that recorded the highest MMRs coming last and to some extent accounting for the rising MMR in the United States between 1900 and 1933. In spite of this complication, however, there is little doubt that the United States experienced one of the highest MMRs in the developed world during the first four decades of the twentieth century.
Figure ΓV.2.3 is a schematic representation of the secular trend in the MMR in various countries between 1880 and 1950. In 1880 the MMR in most developed countries lay somewhere in the range of 50 to 100 deaths per 10,000 births. Between 1880 and 1910, some countries (e.g., Sweden and Belgium) showed a substantial reduction in the MMR, which Hogberg (1985) has suggested was almost certainly the result of the effective use of antisepsis and asepsis. (Although different, both techniques are de
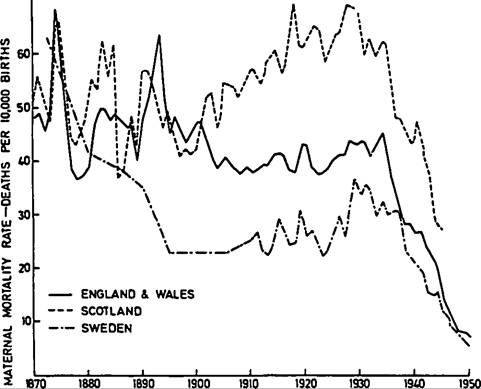
Figure IV.2.4. Maternal mortality rates in Scotland, England, Wales, and Sweden, 1870-1950. (From Annual Reports of the Registrar General for England, Wales, and Scotland. For Sweden, 1860-1910: Ulf Hogberg, Maternal mortality in Sweden, UmeA University Medical Dissertations, New Ser. 156 [UmeA, 1985], 1911-1950: Sveriges Officiella Statistik, Stockholm.)
noted by the term antisepsis in this essay). However, other countries (e.g., Britain and Australia) failed to reduce mortality significantly, a difference that is hard to explain but one that suggests poor antiseptic practice. An example of this difference can be seen in Figure ΓV.2.4, which shows the secular trends in the MMR in Scotland, England and Wales, and Sweden.
That antiseptic techniques, rigorously employed, could be very effective in reducing maternal mortality was beyond doubt. Before 1880, the experiences of lying-in hospitals all over the world were appalling and MMRs of 200 or more were common. By 1900 such hospitals as the Rotunda Hospital in Dublin, the York Road Lying-in Hospital in London, the Matemity Hospital in Basle, and the Women’s Hospital in Sydney reported very low MMRs and a virtual absence of deaths from puerperal sepsis. Such success, however, seems to have been confined to a minority of hospitals, the implication being that those standards of care were the exception before the twentieth century.
This was certainly the belief of the Australian Committee on Maternal Mortality of 1917, which said in no uncertain terms:Puerperal septicaemia is probably the gravest reproach which any civilised nation can by its own negligence offer to itself. It can be prevented by a degree of care which is not excessive or meticulous, requiring only ordinary intelligent and some careful training. It has been abolished in hospitals and it should cease to exist in the community. It should be as rare as sepsis after a surgical operation.
From 1900 to the late 1930s, almost everywhere the MMR stayed level or rose slightly, although there were wide differences among national MMRs. The United States showed the highest and the Netherlands and Scandinavia the lowest. Between 1929 and 1935, the MMR declined slightly in the United States and New Zealand. Elsewhere the trend was level or rising.
When it became obvious that maternal deaths, and especially those from puerperal sepsis, were not being prevented, concern about maternal mortality increased. In many countries, including Britain, Australia, New Zealand, and North America, radical reforms were suggested. These eventually led to improvements in the education and regulation of midwives (except in the United States, where abolition of the midwife was recommended), to better obstetric training for physicians (although in practice little improvement occurred), and an increasing number of specialist obstetricians (with the inevitable tendency for obstetrics to become a branch of operative surgery). Also suggested were the encouragement of routine antenatal care (which seems to have had little effect before the 1940s) and the establishment of new obstetric institutions (clinics, maternity hospitals, and maternity departments in general hospitals in spite of the danger of cross-infection). There were repeated exhortations to use antisepsis properly (which were largely ignored), and local and national governments were urged to improve both the quality and availability of maternal care to women at all levels of society (their actions were usually weak but occasionally effective).
Some medical authorities were optimistic.
Maternal mortality, it was felt, was not a difficult problem. Methods of preventing maternal death were known, and reforms based on them would reduce the tragic and unnecessary loss of so many young women in the prime of their lives. Yet national MMRs showed an obstinate refusal to fall, and a number of studies revealed wide and disturbing regional differences within nations.Map ΓV.2.1 shows regional variations for England and Wales, and Map IV.2.2 the same for the United States. In England and Wales there was a well- marked northwest and southeast divide along a line from the Severn to the Wash, which persisted from the late nineteenth century until the 1930s. Most counties above the line suffered an above-average,
Map IV.2.1. Differences in maternal mortality rates in England and Wales, 1924—33. (From Ministry of Health 1937.)
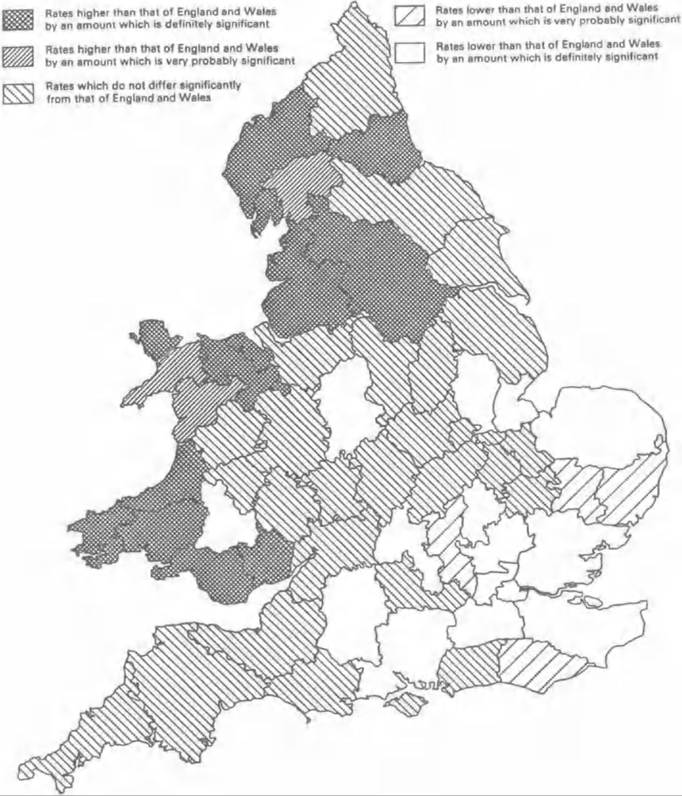
and those below the line a lower-than-average, MMR. The explanation is neither simple nor certain, but it probably lies in the standards of obstetric care rather than standards of living (see the section on determinants).
In the United States the divide was geographically the opposite. Maternal mortality was highest in the South. The states with a high MMR lay along the curve stretching down from Wyoming, Colorado, New Mexico, and Arizona across to the states of the Deep South - Louisiana, Mississippi, Alabama, Florida, Georgia, North and South Carolina, Tennessee, and Virginia. In the Northeast, only Maine showed a persistently high MMR.
The secular trend for the United States as a whole can be seen in Figure ΓV.2.5. The striking features are the high MMRs and the very large difference between white and all mothers, a difference that persisted at least to the 1970s. The high MMR in the South was due largely, but not entirely, to the concentration of the black population. For white mothers as well as black, the MMR was highest in the southern states, but the differential was relatively slight.
In the United States before the Second World War, maternal mortality was usually lower in rural than in urban areas. By the 1960s this situation had been reversed. Remote rural areas, however, often experienced special problems, and wide variations in the provision of maternal care in different parts of the same state were not uncommon. In mountainous areas with deep ravines and few roads, often no trained birth attendants of any kind were available. In other areas, low mortality might be achieved by small homogeneous populations of European origin, which included midwives trained in Europe. Yet other remote areas might possess small local hospitals where nearly all deliveries would be performed by physicians. In many developed countries, a lack of uniformity was the rule rather than the exception as far as factors affecting the MMR were concerned. It was true of Britain, for instance, but most extreme in the United States. In the years 1938-40, when the
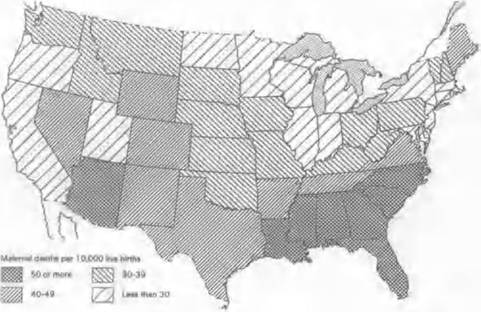
Map ΓV.2.2. Differences in maternal mortality rates in the United States, 1938—40. (From Changes in infant childhood and maternal mortality over the decade 1939— 1948: A graphic analysis, Children’s Bureau Statistical Series, No. 6, Federal Security Agency, Social Security Administration, Children’s Bureau, Washington, D.C.; Infant, fetal and maternal mortality, United States, 1963, National Center for Health Statistics, Series 20, No. 3, U.S. Department of Health, Education and Welfare, Washington, D.C.)
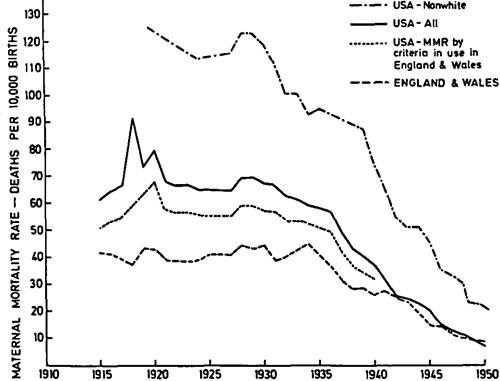
Figure IV.2.5. Maternal mortality rates in England, Wales, and the United States, 1910-50. (From Annual Reports of the Registrar General for England, Wales, and Scotland. For Sweden, 1860-1910: Ulf Hogberg, Maternal mortality in Sweden, UmeS University Medical Dissertations, New Ser. 156 [UmeS 1985], 1911-50: Sveriges Officiella Statistik, Stockholm.
Children’s Bureau Publication. U.S. Dept, of Labor. Washington, D.C., U.S. Govt. Printing Office; R.M. Woodbury, Maternal mortality: The risk of death in childbirth and from all the diseases caused by pregnancy and confinement, Rept. no. 152 [1921]; Elizabeth Tandy, Comparability of maternal mortality rates in the United States and certain foreign countries, Rept. No. 229 [1935].)average MMR for the United States as a whole was 37.6 per 10,000 births, it ranged from 17.5 per 10,000 in North Dakota to 67.8 in South Carolina, a ratio of lowest to highest of 1 to 3.9. In England and Wales in the same period, the average MMR was about 28 per 10,000 and the range between regions was probably about 17 to 38, a ratio of 1 to 2.2.
All this was known to the authorities who made policy in Britain and the United States. Both countries were concerned about their unacceptable MMRs and the obstinately persistent regional differences. But they devised quite different policies. In the United States it was thought that maternal mortality could be defeated by an increase in the proportion of hospital deliveries performed by specialist obstetricians. The midwife and the general practitioner with her or his “kitchen-table midwifery” should be abolished except in remote rural areas.
In Britain it was felt that the backbone of obstetric care should continue to be home deliveries by midwives and general practitioners. Hospital care should increase, but on the whole it should be reserved for complications of labor and high-risk cases. New Zealand tended to follow the U.S. pattern, Australia, the British, and the Netherlands and Scandinavia also pursued a successful policy of home deliveries by midwives backed up by a minimum of hospital deliveries. It is interesting that, in spite of such divergent policies, none of these countries experienced a significant fall in the MMR between 1910 and the mid-1930s.