77 Lead Poisoning
Lead poisoning {plumbism) is defined simply as the undesirable health effects induced by that metal. Many of these, however, are “nonspecific”; that is, they are similar to or identical with symptoms and signs produced by causes other than lead, and some of the toxic effects are so subtle they require laboratory identification.
This historical and geographic discussion concerns itself primarily with those overt effects obviously apparent upon even casual observation by nonmedical observers, which therefore are most likely to appear in the historical record. Principal among these are abdominal colic, muscle paralysis due to lead-damaged nerves, and convulsions.Physiology
Lead gains access to the human body principally through the air we breathe and the substances we ingest. Residents of industrialized nations acquire about half of their “body burden” of lead from polluted respired air. Healthy adults only absorb about 10 percent of ingested lead, but children may absorb as much as half of the lead they eat or drink. Lead absorption is enhanced by a low level of calcium in the diet. Lead may also be absorbed through the skin. Prolonged applications of lead-containing substances such as poultices or cosmetics may result in health-threatening absorption of lead.
Absorbed lead is distributed throughout the body by the blood. The human body’s ability to excrete absorbed lead is so limited, however, that normal life activities in Western countries will produce lead absorption in excess of the body’s excretory capacity. About 5 percent of unexcretable lead is deposited in the liver, brain, and other viscera, where its residence time is only a matter of a few weeks. The other 95 percent is stored in bone for an extraordinarily long time, measurable in decades in the adult. If absorption ceases, such lead will be leached slowly from the skeleton over a period of many years, and is then excreted through the kidneys.
Lead may be transferred to the fetus via the placenta.Methods of exposure to lead as well as the nature of toxic episodes are discussed under History and Geography.
Clinical Manifestations
For many decades the appellation “lead poisoning” has referred to the clinically apparent symptoms manifested by this metal’s toxic effects on the intestine, brain, and nerves. Before dealing with them in detail, however, the less obvious effects of lead poisoning are noted briefly.
Lead can interfere with the physiology of almost every body function. At “low” blood concentration (less than 40 micrograms [μg] Iead/100 ml blood [dl]), there is some evidence that it can impair intellectual capacity development in children, an effect of potentially greater significance for a population than the more overt symptoms usually associated with the concept of lead poisoning. In the mouth, lead may combine with sulfur produced by local bacteria, producing a linear, black precipitate on the gums sufficiently apparent and unique to be of diagnostic value. Episodes of intense lead exposure may cause temporary arrest of long bone growth visible as a horizontal band of radiodensity (“bone lead line”).
Lead produces moderate anemia with resulting facial pallor by poisoning enzymes necessary for the formation of hemoglobin, the blood’s principal oxygen carrier. Lead excreted through the kidneys can poison the renal cells, eventually terminating in fatal renal failure. Effects well documented in animals, though less convincingly in humans, include suppression of gonadal function (with consequent decreased fertility or sterility) as well as carcinogenic and teratogenic activity associated with increased rates of abortion, stillbirth, and neonatal mortality.
The symptom of lead poisoning most commonly encountered in the historical literature is abdominal pain. Its cause is usually attributed to intestinal spasm, though the abdominal muscles may participate in the painful, uncontrolled contractions usually termed “colic.” When they are severe and prolonged, such affected individuals may be driven to desperate measures for relief.
Similar pain may be seen in the common forms of diarrhea, but that associated with lead poisoning is accompanied by constipation, and hence the common reference to the abdominal pain of lead intoxication as “dry bellyache.” In individual cases such a state could be simulated by inflammation of the gallbladder, pancreas, or stomach, and by stones in the kidney or bile passages, but these conditions neither would be accompanied by other symptoms or signs of lead toxicity, nor would they affect large segments of a population or occupation.Lead also has a destructive effect on nerves (peripheral neuropathy), whose ability to transmit the electrical impulses to the muscle is then reduced or completely blocked, producing muscle paralysis. Peculiarly (and diagnostically) the nerves supplying those muscles (extensors), which normally raise the wrist or foot, are especially commonly affected, causing the unique affliction of “wrist drop” (often termed “the dangles” in the past) and “foot drop.”
Serious disturbances of behavior leading to convulsions, coma, and death are the most severe and feared of lead’s effects. Children are notoriously more susceptible to such brain toxicity, and even a single episode of convulsions, when not fatal, often causes permanent, residual cerebral damage. Meningitis, tumors, trauma, and other diseases may result in identical convulsive seizures, and their lead etiology may be recognizable in the literature only through their association with other features of lead toxicity.
Finally it should be noted that lead poisoning may cause gout. This condition is due to the reduced ability of the lead-poisoned kidney to excrete uric acid, a product of normal protein metabolism. The retained uric acid is frequently deposited in the soft tissue, often near joints, resulting in exquisitely tender inflammation. The etiology of the renal toxicity underlying most cases of gout is unknown, but when the kidney injury is caused by lead, it is known as “saturnine gout,” in reference to the association of lead with that planetary god by the ancients.
A rough correlation exists between the amount of lead in the blood and the presence of these various signs and symptoms. At lead levels below 40 μg∕dl, clinically evident effects are uncommon, but with progressively increasing concentrations above 80 μg∕dl, symptoms become more probable. Many modifying and influencing factors, however, give rise to diagnostic difficulties.
Distribution and Incidence
The geographic distribution of lead poisoning is global, but it is not of equal frequency everywhere. Because Circiunstances leading to lead exposure are of anthropogenic origin, the prevalence of plumbism correlates with practices and traditions of lead use. Predictably, the geographic pattern of such episodes has varied with time.
Although there are few recorded instances of major health problems due to lead in antiquity, some perspective on the extent of lead poisoning can be gained by reviewing lead production records. Figure VΠI.77.1 represents an approximation calculated by C. C. Patterson and others. Because galena is the most abundant form of natural lead ore in Europe and Asia, and because its very low solubility produces little toxicity for its miners, one could reasonably surmise that lead poisoning probably was not common prior to the popularization of the smelting process about 3500 B.C.
The cupellation process, discovered about 3000 B.C., permitted the separation of the small amounts of the commonly “contaminating” silver from the much larger quantities of smelted lead, and was followed by a substantial increase in lead production as a by-product of the pursuit of silver in the Mediterranean area. We only speculate about the degree to which lead toxicity affected those involved in lead production in the Middle East and Mediterranean area during these periods, though the crude nature of the furnace facilities must have exposed many to a toxigenic degree.
Introduction of coinage during Greece’s Classical Period resulted in a phenomenal increase in silver (and therefore, lead) production, which was exaggerated by Roman exploitation to the point of ore exhaustion, leading to a marked reduction of that form of mining after the decline of the Roman Empire.
Reference to lead intoxication can be found in the various Greek and Roman writers of antiquity (details under History and Geography: Historical Antiquity). It was then not until the late Middle Ages that lead production rose again, this time in Europe, with recognition of lead’s utility now justifying its acquisition for its own sake. Although the Spanish pursuit of silver in the New World was second only to that of gold, the miners’ mortality was largely due to factors other than poisoning from lead in the ore, and heavy metal toxicity during the silver extraction process was related primarily to the mercury used after 1570. It was the Industrial Revolution, with its enormous surge in lead production, that was responsible for the recurrent endemics in France, Italy, Spain, Germany, and especially Great Britain, and later, their New World colonies. Even so, the 80,000 tons of lead generated annually worldwide at the apex ofFigure VIII.77.1. World lead production during past 5,500 years. [Adapted from Roger L. Boeckx. 1986. Report. Analytical Chemistry 58 (February): 275A, reprinted by permission from Analytical Chemistry, 1986, American Chemical Society.]
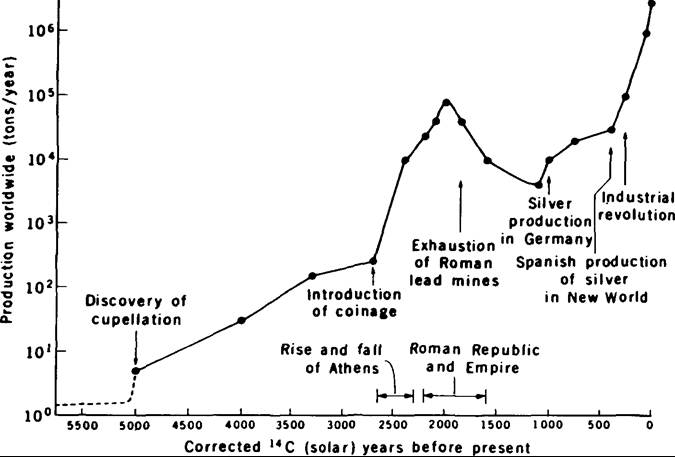
Roman productivity has expanded exponentially to reach more than 3 million tons worldwide today. With this exponential rise has come a staggering degree of lead exposure in the populations of Western nations.
History and Geography
Because various cultures indulged in activities producing serious lead exposure in different periods, this discussion focuses on those periods specifically relevant to lead poisoning.
Prehistory
By definition, this period contains no written record of lead intoxication, but some concept of the extent of lead use and the degree of presumed lead exposure by its consumers is made available by the archaeological record. A few lead pieces from Iraq about 5000 to 4500 B.C.; multiple lead items at the Troy I site; lead tumblers from Mesopotamian tombs; and galena beads in predynastic Egyptian graves from about 3500 to 3000 B.C.; lead pipes at Ur; leaded glazes from Babylon; and leaded bronzes from Thailand between 2000 and 1500 B.C.
- all imply an active, working knowledge of lead smelting. Artifacts also reveal early experimentation with leaded bronzes in China’s ancient metallurgical centers in the southwestern provinces by about 1700 B.C. Skeletal lead analyses by several workers, such as the study by Philippe Grandjean and others (1979) of the Nubian population from as early as 3300 B.C., demonstrate negligible quantities of lead stored in bone, suggesting that lead toxicity in this period was probably limited to the few people directly involved in the smelting process.Historical Antiquity
In Asia Minor, Cappadocian tablets record lead use as an exchange item as early as the third millennium B.C. By 2000 B.C., not only had the smelting of lead ore (conversion to and extraction of metallic lead from the ore compounds) become common knowledge, but also the process of cupellation - the separation of silver from the smelted lead-was widely practiced, as shown by the use of silver as the principal unit of exchange in Susa, Persia, at that time. Old Testament Biblical references testify that lead had broad utilitarian applications and was widely traded even prior to the Israelite departure from Egypt, though there are no comments on its negative health effects. Early dynastic Egyptians used lead for votive statuettes, net sinkers, and cosmetics. Mycenaeans exploited the later well-known mines at Lavrion near Athens and fashioned the product into lead straps. Amulets and loom weights from this period have been found in India. Surely such widespread use of lead must have been accompanied by lead intoxication on occasion, at least among the industrial workers and users of certain lead products including foodwares, but the record remains silent on such matters, implying a probable failure of recognition of its toxic manifestations.
Much of our knowledge about the use of lead in the Greco-Roman period is related to the mines such as the one at Lavrion (called Laurium after the Roman conquest) near Athens. The hilly terrain of the area is laced with intersecting veins of “argentiferous galena,” a lead sulfide ore including as much as 0.5 percent silver as a minor element. This silver was sought by the Athenians, who referred to Lavrion as a “silver mine,” even though they needed to separate 100 to 200 ounces of lead for each ounce of silver retrieved from the ore. This same silver was also one of the sources of Athens’s wealth and power, for with it Themistocles built the navy that defeated the invading Persians and established Athens as the premier Mediterranean sea power. Similar mines were also operated on a number OfMediterranean islands, Asia Minor, and the European continent. Mines have been identified in Spain, France, Italy, and Great Britain. Interestingly, the silver component of ores in England and Wales was so low that these were mined primarily for their lead content.
With the generation of huge quantities of metallic lead as a by-product of the silver refinement process, the obvious utilitarian value of lead was also exploited. Applications included household tableware, storage containers for oil and other fluids, encasement of iron bars to bind construction stones together, sheathing for ships’ hulls, coins, toys, statues, bronze and pewter alloys, coffins, tablets, solder, and a thousand other purposes. During the three centuries of its peak production period, the Lavrion mine is estimated to have yielded over 2 million tons of ore. The most intensive Roman use of lead related to their water system. In addition to lining with sheet lead parts of their extensive aqueductal system and cisterns, Romans also rolled such sheets into tubular form and soldered them to produce pipes through which the water was distributed.
An even more dangerous application of lead lay in its use as a food or beverage container lining and, even worse, as a food additive. In the absence of sugar, Romans used concentrated fruit juice, commonly grape, as a sweetening and flavoring agent (sapa or defrutum). Such juice was concentrated by boiling in lead-lined containers to avoid the undesirable flavor imparted by copper. During the concentration process lead was leached from the container by the acid fruit juice. Replications of this product using original Roman recipes are reported to have resulted in lead concentrations of up to nearly 800 milligrams per liter, about 16,000 times greater than the upper limit for potable water defined by the U.S. Environmental Protection Agency! Eventually Romans acquired such an addiction to the sweet flavor of lead acetate that it was often made available as an optional seasoning additive to wine.
This massive production and utilization of lead in all its forms clearly exposed the majority of urban Romans to lead. Roman customs, however, probably resulted in unequal exposure. Poor and middle-class citizens of Rome and other major communities closely shared ingestion of the lead-contaminated water delivered through the lead-lined aqueducts and pipes of the public water systems. The wealthier class, however, additionally contaminated their wine and food through the more extensive use of lead-lined containers, expensive pewter tableware, and the food additives described above.
It is difficult to imagine that the health problems associated with excessive lead ingestion had not been recognized during this period, and references by contemporary authors indicate many were indeed aware of them. The Greek physician-poet Nicander is normally credited with the first, clear, unequivocal description of plumbism in the second century B.C., when he noted colic, constipation, paralysis, and pallor resulting from the ingestion of the lead compounds litharge and cerusse. Lucretius in the following century described “deadly exhalations of gold and silver mines” and the pallor of miners’ complexions, calling attention to their “short life.” The Roman architect Vitruvius, also in the first century B.C., cautioned that drinking water from surface pools in the vicinity of lead mines was apt to produce muscle cramps and gout. Pliny (first century A.D.) warned against the deadly fumes of silver mines, calling attention to their lethality by their effect on dogs and advising all exposed to such fumes to emulate the miners’ and smelters’ custom of tying an animal bladder over their faces as a mask. Pliny also identified red ■ lead as a deadly poison, whereas his contemporary Celsus described an antidote to white lead. Vitruvius additionally condemned the use of lead for water conduits, noting that lead fumes poison the blood, with consequent pallor as seen in lead workers. Emperor Augustus prohibited the use of lead for water pipes, though there is little evidence of enforcement of his edict. One of the clearest descriptions of lead poisoning affecting large numbers of the population during late Roman times is that by Paul of Aegina, who described an epidemic of colic, lower limb paralysis, and epilepsy in Rome and elsewhere during the seventh century. S. C. Gilfillan (1965) speculated that the well-documented precipitous decline in numbers of the Roman aristocracy during the century following A.D. 60 may have resulted from lead’s toxic effects on fertility (noting that prohibition of wine drinking by women of child-bearing age was lifted about that time) and believes this may have been a major factor in the decline of the Roman Empire. J. Nriagu (1983) suggests further that lead-contaminated wine could explain the bizarre behavior of many Roman emperors and may be the cause of Celsus’s comment that most of them suffered from gout. Although some scholars of Roman history regard the suggestions of Gilfillan and Nriagu as extrapolations beyond available evidence, wine consumption by the wealthy does appear to have increased during the imperial age, and conformity to contemporary suggestions for its preparation would have increased its lead content.
The Industrial Revolution and Modern Europe With the rapid increase in lead production during the Industrial Revolution and the explosive growth that followed, including the modern era of lead fuel additives, the scene of lead poisoning shifted to the European stage. During the sixteenth to the eighteenth and even into the nineteenth century, recurrent waves of tardily recognized lead poisoning epidemics swept the various continental countries and the British Isles, frequently in temporally overlapping inundations. Most of these were eventually traced either to industrial exposure to lead or to ingestion of lead-contaminated beverages or food.
The concept of industrial exposure as a cause of disease was crystallized for eighteenth-century physicians by the masterful studies so meticulously recorded by Bernardino Ramazzini in 1700 (De Morbis Artificum Diatribo), although he was not the first to suggest it. His publications established the clear relationship between certain diseases and occupations. Among them were lead poisoning in miners, potters, and painters.
The French epidemic of crampy abdominal pain termed the “colic of Poitou” began in 1572, but more than a century passed before the consumption of lead-contaminated wine was identified as its etiology. A half-century-long endemic of abdominal colic was initiated in Madrid about 1730. The suggestion that lead was its cause was not taken seriously until 1797, when the fact was made clear that its distribution among the poor was due to their use of badly glazed lead food containers. In the middle of the eighteenth century, Theodore Tronchin realized the “colica pictonum” in Holland constituted poisoning from the use of water draining from lead roofs and from lead water pipes. The eighteenth and nineteenth centuries also were characterized by British importation of Portuguese port wine in prodigious quantities when the 1703 Treaty of Methuen reduced its price to less than that of the French products. The brandy used to fortify the natural wines was often prepared in stills containing lead parts. Such fortified wines are believed to have been responsible for a concurrent frequency of gout so high that this period is often called “the golden age of gout” in England.
Two eighteenth-century workers - Sir George Baker in England and L. Tanquerel des Planches in France - most clearly epitomize publicized recognition of lead ingestion and industrial exposure to lead as the etiology of specific symptom complexes. In the region of Devonshire, England, an epidemic of abdominal colic (“the colic of Devonshire”) raged for decades in the middle of the eighteenth century. Occasional writers had noted its relationship to cider drinking, but its absence in the cider-producing neighboring regions remained puzzling. In 1767, Baker, a Devonshire native, published his report now acknowledged as a milestone in the history of lead poisoning. Baker established the feature that characterized the Devonshire colic: lead contamination of the cider. He had traced the origin of the lead to a type of millstone used in the cider’s manufacturing process. The Devonshire millstones were unique in that they were made in multiple segments bonded together by lead keys exposed on the stone’s surface. He also noted the custom of cider storage in lead- lined containers and the addition of lead to the cider as a flavoring and preservative agent. His publication, clearly indicting lead as the epidemic’s cause, was followed by preventive practices and a gradual subsidence of the epidemic.
Similarly, for many decades in the eighteenth and early nineteenth centuries, Paris’s Charity Hospital had become famous for its treatment of patients with the various “dry colic” syndromes. In 1839 Tanque- rel des Planches reported how he had studied these patients’ complaints, scoured their hospital charts, and eventually demonstrated that most were engaged in an occupation involving unequivocal lead exposure. His detailed clinical observations included paralysis, encephalomalacia, and such a thorough description of the other items comprising the lead poisoning syndrome that it can be used as a medical teaching exercise today.
The New World Colonial Period
There was hardly a pause in the spread of the European colics before they also appeared in the American colonies. These settlers had arrived in the New World with a restricted hoard of tools and machinery; malleable lead could be and was employed to create substitutes for a myriad of items manufactured out of steel in Europe with consequent opportunities for lead exposure.
One such source exposure was the consumption of lead-contaminated liquor. The coiled condensation tube (usually called the “worm”) of an alcohol still was most easily fashioned out of lead. The distillation of fermented sugar products in such a still for rum production caused sufficient lead leaching from the “worm” to render the rum toxic. By 1685, epidemics of abdominal colic (“dry bellyache” or “dry gripes”) were common in North Carolina and Virginia. Upon suggestions from those consumers that their illness might be the result of lead-contaminated New England rum, Massachusetts protected its trade market with remarkable alacrity by enacting the Massachusetts Bay Law of 1723, prohibiting the use of lead parts in a liquor distillation apparatus. Although the law is often hailed as the first public health law in the colonies, it should be noted there is no evidence of any serious, objective investigation regarding the role of lead in the origin of the rum-drinkers’ symptoms, nor does the medical profession seem to have been the principal instigator for the law’s passage. It appears the legislators were responding primarily to customer complaints, motivated more by trade than by health concerns.
Both the continent and the West Indies had a similar problem. Whereas slaves on North American continental plantations developed lead poisoning infrequently, the afflicted individuals on Caribbean island plantations included both Caucasians and black slaves. Barbados was especially affected, with the literature from the latter seventeenth and much of the eighteenth centuries replete with references to “dry bellyache,” clearly a clinical entity well known to both physicians and the laity but of undetermined cause. Jerome Handler and others (1986) provided the chemical support for the diagnosis of lead poisoning in the slaves of a Barbadian population from the eighteenth century by finding sufficient lead in their archaeologically excavated bones to predict that at least one-third of them probably had had lead poisoning symptoms of moderate or greater severity.
The reason for high bone lead values in island plantation slaves in contrast to those on continental plantations lay in the nature of the product: sugar in the islands; cotton, fruit, or tobacco on the continent. The sugar was collected in lead-lined tubs, ducted through lead pipes into a lead-lined copper cauldron in the boiling-house (whose fumes would expose the boiling-house workers), and stored in lead containers, to be distilled later into rum through a lead still. In addition, the lead-laden rum was used as a work incentive with subsequent consumption in large quantities of this lead-contaminated liquor by the afflicted slaves.
In 1745 Benjamin Franklin published Thomas Cadawaler’s treatise on dry gripes in which the role of lead was defined. This knowledge may have been carried to Europe by Franklin because Baker of Devonshire quoted Franklin in his well-known 1767 article. By the mid-eighteenth century, knowledge about the lead etiology of the dry bellyache was reaching Barbados. In 1788 John Hunter (Observations on the Diseases of the Army in Jamaica) detailed dry gripes symptoms and specifically attributed them to lead. The condition gradually subsided in the West Indies during the last quarter of the century.
Another common source of lead poisoning in colonial America was houseware, especially those items used in the preparation, serving, or storage of food and beverages. In England, expensive pewterware, some with more than 20 percent lead composition, was the symbol of social and economic success, and this was emulated in the colonies. Plates and goblets were commonly of pewter in the wealthier colonial homes; perishables such as milk, cream, or fruit juices were stored in lead-lined containers as were wine, drinking water, and other beverages. Indeed, in such a wealthy home almost everything the family ate or drank contained some lead. In a continental plantation where access to such lead-contaminated food was tightly controlled, Arthur Aufderheide and colleagues (1981) could demonstrate that the extent of differential lead exposure had a socioeconomic basis. The slave labor force of a 1670-1730 Virginia plantation had no more lead in their bones than the average, modern North American does, but the skeletons of their wealthy Caucasian masters contained a sixfold greater quantity. Colonists were also exposed through their use of lead bottles, funnels, nipple shields, dram cups, candlesticks, lamps, pipes, roof gutters, and many other items.
Mining also claimed its colonial victims. The eastern American mines were largely of the poorly soluble galena ore and generated little morbidity. It was in the western Utah mines, whose ore was predominantly lead carbonate, that lead poisoning reached epidemic proportions, with many thousands of miners suffering from plumbism between 1870 and 1900.
The Present Era
Even though we have a more sophisticated understanding of lead poisoning today, our ongoing use of lead seems to provide new opportunities for exposure. Lead encephalopathy acquired by infants nursing at the breasts of mothers using lead-containing cosmetics constituted the fourth most common, fatal, pediatric malady in Manchuria in 1925. A poisoning episode from lead fumes occurred in a Baltimore neighborhood in 1933 when poor families there burned discarded battery casings as cheap fuel. Until C. C. Patterson (1982) called attention to it recently, lead solder was used to seal many food cans. The common practice of pica (dirt eating), partly biological and partly cultural in origin, has become especially dangerous for children playing in yards whose soils are badly contaminated from inner-city factory and vehicle-exhausted lead. Chips of leadladen, old paint peeling from their aging houses constitute a toxic time bomb for the very young. Many surviving victims of childhood lead poisoning in Australia were found to suffer failure of Iead- poisoned kidneys several decades later. A 1910 American pharmacopoeia still listed both a variety of therapeutic lead compounds and antidotes to lead poisoning! There is probably no purer example of the price exacted by historical ignorance than the plumbism rampant among the modern illicit liquor producers (“moonshiners”) using lead-containing distillation units (automobile radiators soldered with lead) in the United States today.
American lead production peaked about 1975, with at least half of it converted into automobile fuel additive. Recent partial control of automobile exhaust fumes has been accompanied by a 37 percent reduction in average blood lead levels in Americans.
Statistical data for lead poisoning are difficult to acquire, but in the United States, 831 adult deaths could be identified between 1931 and 1940; whereas in England, Tony Waldron (1982) describes a reduction from about 115 deaths annually in 1900 to only an occasional few by 1960. In view of the known diagnostic inefficiency of lead poisoning, these are surely minimal figures.
Prevention and Control
For many centuries, humanity’s flirtation with lead frequently has been its undoing. Its romance with this pedestrian metal has been inspired not by any gemlike allure it possesses but, rather, by its irresistible utility. No other metal is so easily extracted from the soil and so readily fashioned into unlimited numbers of needed items. In every age, however, writers sounding the warning of its toxic hazards were ignored or decried. Reasons for such resistance remain enigmatic.
It may be that the nonspecificity of the lead intoxication syndrome confused earlier diagnosticians because other conditions can simulate some of lead’s toxic effects. The mine fumes that several Greco- Roman period authors held responsible for lead miners’ health problems were perhaps the obvious and unpleasant sulfur dioxide odors emitted by galena ore rather than by lead compounds. Yet Pliny even complained specifically that the practice of “adulterating” wine (adding lead to improve the flavor) produces nerve injury manifested by paralyzed, dangling hands. His contemporary, the physician Dios- corides, clearly described colic and renal failure resulting from drinking the lead oxide compound called litharge. Most ancient miners were slaves whose ailments may not have been treated by physicians. It is, of course, possible that Romans were not exposed to as much lead as we presume today and that a lack of concern by Roman physicians simply reflects a low frequency of lead poisoning in ancient times. This can be evaluated objectively only by lead analysis of appropriately selected ancient bones. To date, some of Waldron’s (1982) Romano-British cemetery excavation studies have revealed elevated bone lead values, but further investigations on Italian samples with sharply defined socioeconomic status of the studied individuals will be needed to resolve this question.
Perhaps even more relevant is the fact that during most of history the cause-and-effect relationship between a specific agent like lead and a specific symptom was only vaguely appreciated by physicians whose theoretical concepts did not readily embrace such an association. More concerned with the balance of postulated body humors, they were apt to attribute a broad range of symptoms to general environmental (often climatic) disturbances. Even nineteenth-century French naval surgeons accepted lead as the etiology of the lead poisoning syndrome but rejected it as the cause of an identical symptom complex in their tropical sailors. They attributed it instead to the effect of high tropical temperatures, thus delaying recognition of its true origin in their custom of shipboard food storage in lead containers.
Surely, lack of a system for regular publication and wide dissemination of medical knowledge also contributed to delay in grasping the etiology of lead poisoning. As early as 1656, Samuel Stockhausen, a physician to the lead miners of northern Germany, published his realization that their affliction was the toxic effect of the lead ore they mined. Forty years later, that observation led his south German colleague, Eberhard Gockel, to recognize lead contamination of wine as the cause of an identical problem in his clerical patients, and it was to be more than another century (and many more “colic- demics”) before the translation of Stockhausen’s report into French enabled Tanquerel to identify the same problem at Paris’s Charity Hospital.
JosefEisinger (1982) has noted the recurring need throughout most of Western history for governments to enact legislation restricting the population’s exposure to lead. Serious and major efforts to reduce lead exposure, such as the 1971 Lead-Based Poisoning Prevention Act in the United States and more recent legislation involving lead air pollution by automobiles, are phenomena primarily since the 1970s. The history of the past two millennia, however, suggests that our knowledge of lead’s potential hazards will not prevent at least some continuing problems with its health effects.
Arthur C. Aufderheide
Bibliography
Aufderheide, A. C., et al. 1981. Lead in bone II. Skeletal- lead content as an indicator of lifetime lead ingestion and the social correlates in an archaeological population. American Journal of Physical Anthropology 55: 285-91.
Boeckx, Roger L. 1986. Report. Analytical Chemistry 58(2): 275A.
Eisinger, J. 1982. Eberhard Gockel and the colica Pictonum. Medical History 26: 279-302.
Gifillan, S. C. 1965. Lead poisoning and the fall of Rome. Journal of Occupational Medicine 7: 53-60.
Gockel, Eberhard. 1697. Eine curiose Beschreibung dess An 1694.95 und 96 durch Silberglett Versussten sau- ren Weins.... Ulm.
Grandjean, Philippe, O. Vag Nielson, and Irving M. Shapiro. 1979. Lead retention in ancient Nubian and contemporary populations. Journal OfEnvironmental Pathology and Toxicology 2: 781—7.
Handler, J. S., et al. 1986. Lead contact and poisoning in Barbados slaves: Historical, chemical, and biological evidence. Social Science History 10: 399-425.
Hirsch, August. 1883-6. Handbook Ofgeographic and historical pathology, 3 vols. London.
McCord, C. P. 1953.1954. Lead and lead poisoning in early America. Industrial Medicine and Surgery 22: 393-9, 534-9, 573-7; 23: 27-31, 75-80,120-4,169-72.
Nriagu, J. 1983. Lead and lead poisoning in antiquity. New York.
Patterson, Clair C. 1982. Natural levels of lead in humans. California Environment Essay, Ser. 3, Institute for Environmental Studies, University of North Carolina. Chapel Hill.
Stockhausen, Samuel. 1656. Libellus de Hthargyrii fuτno noxio morbifico, metallico frequentiori morbo vulgo dilto Die Huettenkatze. Goslar.
Waldron, H. A., and D. Stofen. 1974. Subclinical lead poisoning. London.
Waldron, Tony. 1982. Human bone lead concentrations. In Romano-British cemeteries at Circencester, ed. Alan McWhirr, Linda Viner, and Calvin Wells, 203-4. Circencester, England.