76 Lassa Fever
Recognition of Africa’s major endemic diseases of human beings was apparently well advanced by 1900. Malaria, trypanosomiasis, yellow fever, schistosomiasis, typhoid fever, brucellosis, and a long list of other afflictions had been characterized.
But then, in 1969, a new member of the coterie of major endemic diseases of Africa entered the scene: Lassa fever.The events leading to the discovery were dramatic. A nurse, Laura Wine, in a mission hospital in Lassa, Nigeria, became ill, progressed unfavorably, and died, despite the marshaling of antimalarials, antibiotics, antimicrobial agents, and supportive therapy. This death, as a statistic, would probably have been labeled “malaria” and thus been registered as such in national and World Health Organization disease records. But another nurse, Charlotte Shaw, who attended the first, also became ill. She was taken by small plane from Lassa to the Evangel Hospital in Jos, Nigeria, operated by the Sudan Interior Mission, where she died while being attended by physicians Harold White and Janet Troup, and nurse Lily Pinneo. Again, there was no firm diagnosis. Pinneo then got sick. Doctors at the hospital were thoroughly alarmed. She was evacuated, via Jos and Lagos, to America by plane, and was admitted to the College of Physicians and Surgeons at Columbia University, where she was attended by John Frame, E. Leifer, and D. J. Goeke.
The Yale Arbovirus Research Unit in New Haven, Connecticut, was alerted by Frame, who helped to get specimens for the unit. By a combination of serendipity and skill, an agent was isolated — a virus, unknown hitherto to humans. It was called “Lassa virus” (Buckley, Casals, and Downs 1970). Two laboratory-acquired cases occurred in Yale personnel working on the virus. One of them, Juan Roman, died. The other, Jordi Casals, was given immune plasma from the recently recovered nurse, Pinneo, and made a full recovery.
In due course and with unfailing collaboration from many services, the agent was established as belonging to a grouping including lymphocytic choriomeningitis virus of nearly worldwide distribution. (Examples are Taca- ribe virus from bats in Trinidad; Junin virus, the causative agent of Argentine hemorrhagic fever; and Machupo virus, causative agent of Bolivian hemorrhagic fever.) The grouping of these agents hasTable VIII.76.1. Lassa fever outbreaks: West Africa, 1969-88
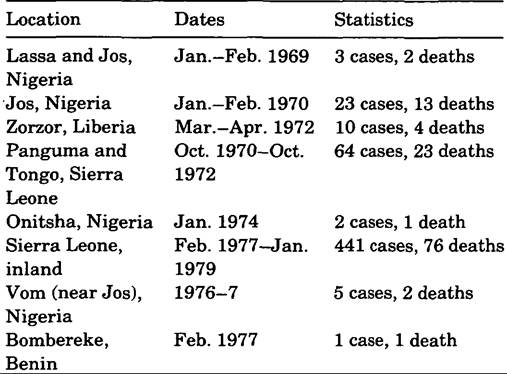
Note: Seropositive individuals have been detected in Senegal, Guinea, Central African Republic, and the Camer- oons.
been officially designated Arenavirus in the family Arenaviridae (Fenner 1976). As portrayed in Table VIII.76.1, seven other outbreaks of Lassa fever are known to have occurred in Africa since 1969. Unfortunately, Nurse Troup, who attended cases in the 1969 outbreak at Jos, became infected through a finger prick in an outbreak at Jos the following year and died.
Clinical Manifestations, Morbidity, and Mortality
High fever associated with malaise, muscle and joint pains, sore throat, retrosternal pain, nausea, manifestation of liver involvement, bleeding tendency of variable severity, proteinuria, and erythematous maculopapular rash with petechiae are features of the illness, but not of themselves particularly diagnostic. The presence of an enanthem in the oropharynx has been considered by some to have specific diagnostic importance.
In early stages, the disease can simulate many illnesses occurring in Central Africa, prominent among them malaria (Downs 1975), although typhoid fever, rickettsial diseases, brucellosis, hepatitis (before appearance of jaundice), and even yellow fever can also be mimicked. Sporadically occurring Lassa cases are certainly not often diagnosed. When epidemics arise, the clumping of cases of mysterious illness can and has attracted attention, leading to diagnosis.
It has become recognized from studies, such as one in Sierra Leone, that there are many mild Lassa cases (McCormick et al. 1987a). This study of several years’ duration was conducted by personnel from the Centers for Disease Control, U.S. Public Health Service, in two hospitals in central Sierra Leone. It determined that Lassa was the causative agent (determined by virus isolation) in 10 to 16 percent of all adult medical hospital admissions and in about 30 percent of adult hospital deaths. The fatality rate for 441 hospitalized patients was 16.5 percent.Karl M. Johnson and colleagues (1987) have shown that mortality is directly associated with level of viremia, although it must be noted that by the time figures for viremia have been received from the overseas laboratory, the patient is either recovered or dead. Joseph B. McCormick and colleagues (1987b) estimate the ratio of fatalities in infections in general to be 1 to 2 percent, a rate lower than estimates based on hospitalized patients. How widely the findings on rates and outcome can be extrapolated to other hospitals and other settings in West Africa is not yet known. Studies simply have not been done to determine this. However, it is clear that when seriously ill patients are seen, the prognosis is highly unfavorable, even when the best of currently recognized therapeutic regimes are applied.
Virus Morphology, Size, and Structure
F. A. Murphy and S. G. Whitfield (1975) have given a detailed account of the morphology and morphogenesis of the virion and have related it to the other members of the Arenavirus group. The virus particles, on budding from the cell membrane, may be round, oval, or pleomorphic, with mean diameters of 110 to 130 nanometers and with spike-covered envelopes. The center of the particle contains variable numbers of fine granulations, measuring 20 to 25 nanometers, a characteristic that prompted the name Arenavirus. The nucleosome consists of singlestranded RNA. In 1984, F.
Lehmann-Grube furnished a detailed account of the development and pathogenetic characteristics of the Arenaviridae.Diagnosis
Laboratory findings include leukopenia and increasing thrombocytopenia, proteinuria, and hematuria, and evidence of coagulation. Diagnostic tests have been developed. Viremia is a constant feature in Lassa cases, and the virus can be isolated and identified in cell culture, using procedures that take a week or more to run. By this time, the patient, if indeed a Lassa patient, may be in dire straits. A rapid diagnostic test is sorely needed. Progress has been made in survey methodology. Serum specimens from suspected patients, taken a few weeks after illness, and those taken in samplings of populations, can be examined for the presence of antibody to Lassa, using a special test plate developed in U.S. Army laboratories. “Spots” of inactivated antigens are made on a test plate, called colloquially a CRELMplate. A drop of serum from an individual is placed on each of the “spots” of, respectively, Congo-Crimean fever, Rift Valley fever, and Ebola, Lassa, and Marburg inactivated viruses, and incubated. A fluorescein-tagged anti-human globulin is then added to each drop. Development of fluorescence in one of the “spots” after incubation indicates presence of human antibody, coupled to the signaled antigen. This method has led to greater knowledge of several deadly diseases in Africa, and is a major step toward understanding the geographic location of these diseases.
Treatment
Treatment modalities are being explored. Ribavirin shows promise of benefits if administered early enough in the course of disease (McCormick et al. 1987a,b). An early hope in treatment, administration of plasma from recovered cases, has not been very successful. If given early enough, before a positive laboratory diagnosis is possible, it may have some value. Given later, there have been occasional dramatic recoveries, as in the case of Yale’s Jordi Casals.
But there have also been many failures. Renal shutdown has been a fatal feature of such treatment in some instances. All work with Lassa virus must be conducted under conditions of highest security (MMWR 1983), which slows down laboratory work. Several human deaths have occurred among laboratory workers, nonetheless.Epidemiology
The association with the Arenavirus group helped to orient the studies in Africa, relating to determination of the transmission cycle of the Lassa virus. Predictably, like its congeners, it was determined to be an infection of small rodents, usually housefrequenting rodents. Praomys (Mastomys) natalen- sis in sub-Saharan, equatorial, and southern Africa is the most common house-frequenting rodent and has been found infected to varying degrees in several regions in Africa afflicted with Lassa (McCormick et al. 1987a,b). The infection in the rodent is persistent, with virus in the urine a common feature. As epidemics occurred in other localities in Nigeria, Liberia, and Sierra Leone over the course of several years, it became apparent that Lassa virus is widespread in West Africa and also may be found in East Africa (McCormick et al. 1987). Studies of distribution are far from complete.
Control
Control must proceed at several levels. At the village level, community-wide rodent control may be implemented, which should include rodent proofing of grain storage facilities, general trash cleanup, and rodent poisoning campaigns. At the householder’s level, measures should include rodent proofing of dwellings, rodent trapping, and rodent poisoning. At the clinic level, the possibility of Lassa should be considered whenever fever cases are seen, and appropriate measures taken to protect the examiner and other patients at the clinic. At the hospital level, attention must be given to rodent control, and in addition, diagnosed or suspected Lassa patients should be isolated, with staff taking full precautions to avoid close contact with them.
Special precautionary measures are indicated for obstetrical, gynecological, and surgical services. At the governmental level, Lassa should be made a reportable disease, and at the international level, Lassa must be made a reportable disease.Wilbur G. Downs
Bibliography
Auperin, David D., and Joseph B. McCormick. 1989. Nucleotide sequence of the Lassa virus (Josiah strain) S genome RNA and amino acid sequence of the N and GPC proteins to other arenaviruses. Virology 168: 421-5.
Buckley, Sonya M., Jordi Casals, and Wilbur G. Downs. 1970. Isolation and antigenic characterization: Lassa virus. Nature 227:174.
Downs, Wilbur G. 1975. Malaria: The great umbrella. Bulletin of the New York Academy of Medicine 51: 984-90.
Fenner, Frank. 1976. Classification and nomenclature of viruses. Second Report of the International Committee on Taxonomy of Viruses: Intervirology 7: 1-116.
Fuller, John G. 1974. Fever: The hunt for a new killer virus. New York.
Johnson, Karl M., et al. 1987. Clinical virology of Lassa fever in hospitalized patients. Journal of Infectious Diseases 155: 456-64.
McCormick, Joseph B., et al. 1987a. A case-control study of the clinical diagnosis and course of Lassa fever. Journal of Infectious Diseases 155: 445—55.
1987b. A prospective study of the epidemiology and ecology of Lassa fever. Journal of Infectious Diseases 155: 437-44.
MMWR. 1983. Viral hemorrhagic fever: Initial management of suspected and confirmed cases. Morbidity and Mortality Weekly Report Supplement 32, No. 2S: 27S— 39S.
Murphy, Fred A., and S. G. Whitfield. 1975. Morphology and morphogenesis of arenaviruses. Bulletin of the World Health Organization 52: 409—19.
Saltzmann, Samuel. 1978. La Figure de Lassa. Editions des Groupes Missionnaires. Annemasse, France.
Vella, Ethelwald L. 1985. Exotic new disease: A review of the emergent viral hemorrhagic fevers. United Kingdom Ministry of Defence. Section One: Lassa fever — the multimammate rat disease.