75 Lactose Intolerance and Malabsorption
Lactose malabsorption describes a physiological situation. It is the basis for lactose intolerance. The inability to digest lactose is a quantitative phenomenon related to the enzyme lactase and its amount and activity in the intestine.
Lactose intolerance, then, is a clinical definition. It involves the concept that the individual is unable to tolerate physiologically the lactose present in milk and other dietary products because of an inability to digest the carbohydrate, due to insufficient activity of the lactase enzyme. Intolerance to lactose as a clinical entity has been recognized for some time. Early in this century, Abraham Jacoby hinted at the existence of lactose intolerance in speeches to the American Pediatric Society; later, in 1926, John Howland, in his presidential address to that same organization, was somewhat more explicit when he indicated that many of the infantile diarrheas were the result of a lack of “ferments” necessary for the digestion of carbohydrate (Flatz 1989).More recently, interest of physicians and nutritionists in the digestion of lactose stimulated reports during the late 1950s. One by A. Holzel and colleagues (1959) reported on a severe diarrhea associated with the ingestion of lactose in two young siblings who, as a consequence, were “failing to thrive.” Another report, by P. Durand (1958), diagnosed two patients with lactose malabsorption and Iactosuria. Since then, innumerable articles and reviews have appeared in the world’s literature (Scrimshaw and Murray 1988). Evaluations of that literature may be obtained by consulting G. Semenza and S. Auricchio (1989), G. Flatz (1989), and N. Kretchmer (1971).
Lactose: Chemistry, Digestion, and Metabolism
Lactose is a galactoside composed of glucose and galactose. This compound is found in the milk of most mammals, although in marsupials and mono- tremes it appears in conjugated form.
It is entirely lacking in the milk of the California sea lion and related pinnipedia of the Pacific Basin. The reason for the latter is that lactose is synthesized in the mammary gland from two monosaccharides, glucose and galactose, by the enzyme galactosyltransferase, which requires the presence of alpha-lactalbumin - not produced by the mammary glands of the sea lion. Thus the concentration of lactose in the milk of placental animals ranges from a low of zero to a high of 7 percent (Sunshine and Kretchmer 1964).Lactose is digested in the small intestine by the lactase (a galactosidase), which is located in the brush border of the epithelial cells of intestinal villi. This enzyme is anchored to the membrane by a hydrophobic tail of amino acids. Detailed descriptions have recently been published of the intimate intracellular metabolism of lactase (Castillo et al. 1989; Quan et al. 1990).
In most mammals the activity of lactose-digesting lactase is high during the perinatal period; after weaning the activity declines to about 10 percent of its original value. But in certain human groups the enzyme activity remains elevated throughout the lifetime of most of their members (Kretchmer 1977). Examples of these groups include northern Europeans, people of Magyar-Finnish extraction, and two African tribes, the Fulani and the Tussi.
Clinical Manifestations
The clinical manifestations of lactose intolerance include increasing abdominal discomfort, borboryg- mus, flatulence, and finally fermentative diarrhea. Although an inordinate amount of any carbohydrate in the diet will produce a similar symptomatology, intolerance to lactose is the most prominent of these clinical syndromes. The basis of this phenomenon is primarily the activity of the lactase relative to dietary lactose. The lower the activity, the less the capacity for the hydrolysis of the lactose, although other factors - such as intestinal motility and the presence of other nutrients — also play a role in this phenomenon.
When the capacity of the lactase is exceeded, the nonhydrolyzed dietary lactose passes into the large bowel where it is fermented by the myriad of colonic bacteria. This action in turn yields propionic acid, hydrogen, methane, and alcohols, and results in a watery diarrhea, the pH of which is acidic.
In general, the activity of lactase in the intestine in almost all mammals by the time of weaning has decreased to about 10 percent of that encountered during the perinatal period. This does not mean, however, that weaning is directly related to the decrease in activity of lactase. There has been no documentation indicating that there is any inductive relationship between the activity of the enzyme and the ingestion of milk. In fact, all the careful studies indicate that there is no relationship between the two events (i.e., the ingestion of milk and the activity of lactase).
Classification
Lactose malabsorption can be classified into three categories:
1. Congenital malabsorption of lactase, a rare phenomenon, which has been documented in only a few cases.
2. Primary malabsorption of lactose, a worldwide situation that is encountered in humans after the age of 5 to 7 years, and in other animals after weaning. (This is considered to be a normal physiological process, transmitted genetically; indeed it resembles a classical Mendelian recessive trait.)
3. An acquired malabsorption of lactose that can be encountered at any age in infants and children under 7 years, as well as in adults who had previously been lactose absorbers. This form can also be associated with nonspecific and specific diarrhea of infancy, drugs that affect the intestinal mucosa, and diseases such as cystic fibrosis and gluten-sensitive enteropathy.
An interesting phenomenon is that the colonic flora of the lactose-intolerant individual seems able to adapt to a nonfermentive type of bacteria. A study was launched in Nigeria in which six medical students, all proven lactose nondigesters, were fed graded doses of 5 grams of lactose to a final amount of 50 grams over a 6-month period.
At the end of this time, all six of the individuals could tolerate the 50 grams of lactose, but were shown to be unable to digest it. Adults who should be intolerant to lactose can drink a glass, or even a pint, of milk with relative impunity, but nonetheless manifest no increase in lactase activity and consequently cannot digest the lactose.History and Geography
The ability to digest lactose is a nutritional event that can be clearly associated with evolutionary pressures. During the Neolithic period, human adults began to drink milk, probably in association with the domestication of animals. These ancient pasto-
ralists who originated in the Euphrates River Valley were nomadic, constantly in search of new pastures for their animals. It is assumed that they migrated in two main directions: to the northwest, toward Europe; and to the southwest, across the then-fertile Sahara toward east and west Central Africa. The exact time of these migrations is unknown, but presumably the nomadic pastoralists of Africa (e.g., the Fulani, the Tussi, the Masai, and others) have their origins in these migrations as do those of northern Europe.
In the Americas, by contrast, there were no indigenous pastoral groups, and thus, in the Western Hemisphere, there was no ingestion of milk after weaning until the Europeans arrived. An absence of dietary milk after weaning was also the case in Australia, the islands of the Pacific, Japan, and the rest of Asia. In these regions the individual after weaning obtained calcium from small bones, limestone, darkgreen vegetables, and fermented or pressed (and thus much reduced in lactose) dairy products.
Thus the present-day geographic distribution of peoples who can or cannot digest lactose fits with our historical knowledge of the distribution of ancient pastoral groups and the milking of their animals. Nonetheless, confusion arises over questions of levels of lactose intolerance among peoples with no history of pastoral activity.
In the case of a native American population - the Pima-Papagos, for example - the inability to digest lactose has been reported at only 60 percent (see Tables VIII.75.1 and VIII.75.2). The 40Table VIII.75.2. Distribution of the adult lactase phenotypes in human populations
Table VIII.75.1. Lactose absorption and malabsorption correlated with degree of Indian blood (children ≥4 years, and adults)
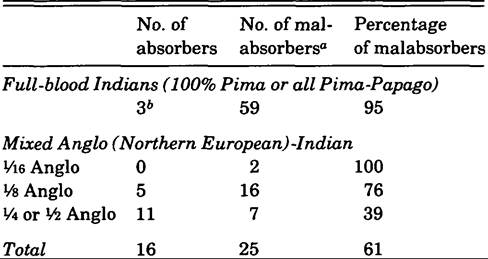
oMalabsorbers represent 21 adults (> 18 years), 38 children (4-18 years).
6Ages 4, 4½, and 6 years.
Source: Johnson et al. 1977. Lactose malabsorption among the Pima Indians of Arizona. Gastroenterology 73(6): 1229-1304, p. 1391, by permission of Gastroenterology.
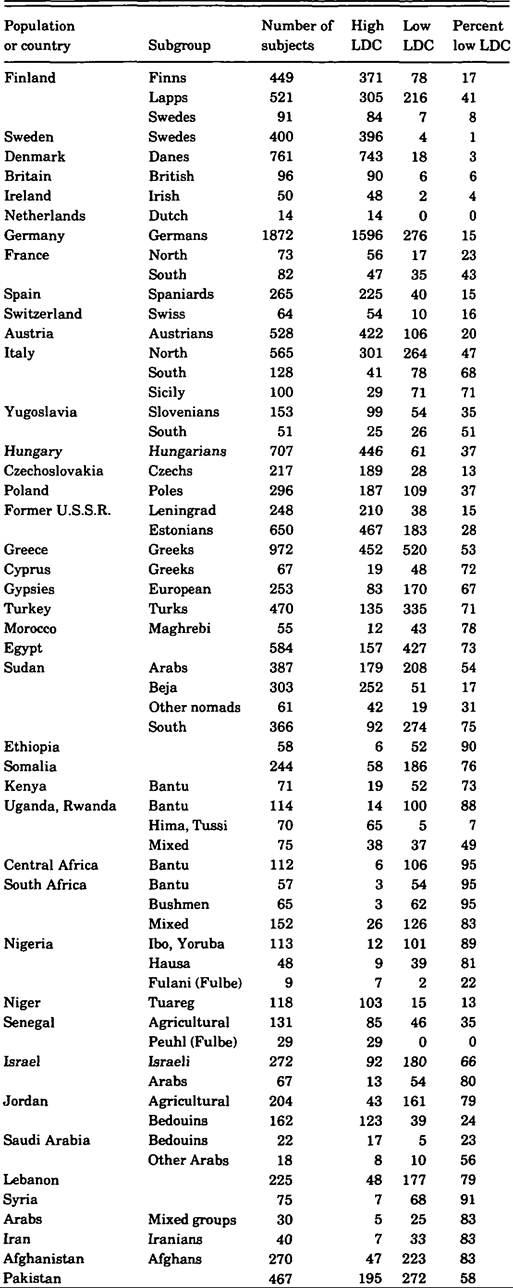
Table VIII.75.2. (cont.)
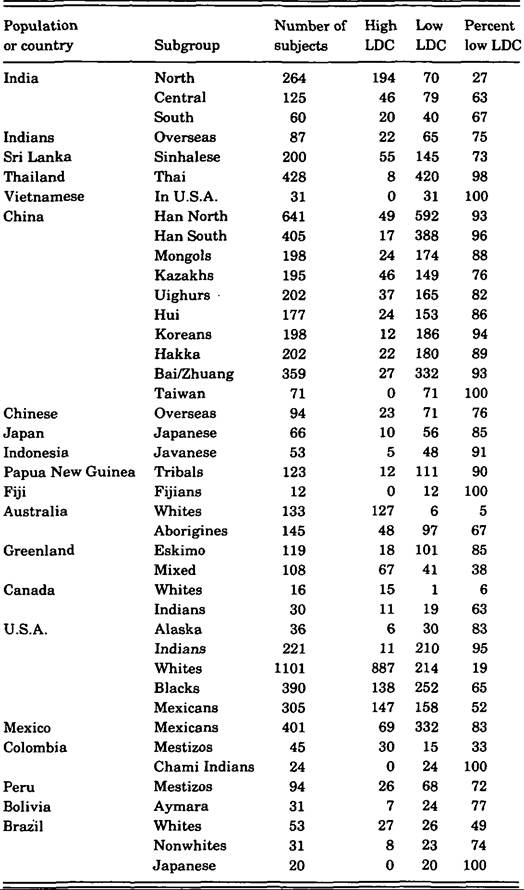
Note: LDC = lactose digestion capacity.
Source: G. Flatz. 1989. The genetic polymorphism Ofintestinal lactase activity in adult humans. In The metabolic basis of inherited disease, 6th edition, ed. G. R. Scriver, A. Z. Beaudet, W. S. Sly, and D. Valle, ρ. 3003. New York. By permission OfMcGraw-Hill B∞k Company.
percent who can drink milk, however, represent the genetic penetrance of the pure genetic pool of native Americans with a gene that affords them the ability to digest lactose. Without that genetic penetrance, the percentage that could not digest lactose would have reached 100.
Flatz (1989) has compiled a list of figures that report the distribution of lactose phenotypes for many populations of the world (see Table VII.75.2). These data support the cultural hypothesis first promulgated by Frederick Simoons (1970), which states that the ability to digest lactose is associated only with a population that has a history of pastoralism.
The hereditary pattern for the ability to digest lactose appears to be simple and to follow straightforward Mendelian genetics. The individual who can digest lactose carries the mutated gene, which in this case, is dominant. The lactose nonabsorber carries a recessive gene. Consequently, the cross between lactose malabsorbers always yields progeny who are lactose malabsorbers, thus perpetuating the absolute inability to digest lactose among a lactose- intolerant population.Summary
Lactase has been shown in a number of careful investigations to be the same enzyme in the infant as in the adult who can digest lactose, and in the residual activity found in the nondigester. In general, the lactose digester has 10 times more enzymatic activity than the lactose nondigester. Thus, the biochemical genetics of lactose digestion is related to the amount and activity of lactase.
Today, lactose malabsorbers who would like to be able to drink milk can purchase various “lactase” preparations now on the market that “digest” the lactose in milk before it is ingested. Others who do not drink milk can overcome the potential dietary calcium deficiency by consuming fermented milks, pressed cheeses, dark-green vegetables, and small bones as in sardines.
The worldwide distribution of an inability to digest lactose after weaning in most human adults and all other mammals argues for this condition to be the normal physiological state. The ability to digest lactose would seem then to be evidence of a genetic polymorphism. It is only the bias of the milk-oriented societies of northern Europe and North America that casts lactose malabsorption as an abnormality.
Norman Kretchmer
Bibliography
Castillo, R., et al. 1990. Intestinal lactase in the neonatal rat. Journal of Biological Chemistry 265: 15889—93.
Debongnie, J. C., et al. 1975. Absorption of nitrogen and fat. Archives of the Diseases of Childhood 50: 363-6.
Durand, P. 1958. Idiopathic Iactosuria in a patient with chronic diarrhea and acidosis. Minerva Pediatrica 10: 1083-1147.
Flatz, G. 1989. The genetic polymorphism of intestinal lactase activity in adult humans. In The metabolic basis Ofinherited disease, 6th edition, ed. C. R. Scriver et al. New York.
Holzel, A., V. Schwartz, and K. W. Sutcliff. 1959. Defective lactose absorption causing malnutrition in infancy. Lancet 1: 1126—8.
Johnson, J., et al. Lactose malabsorption among the Pima Indians of Arizona. Gastroenterology 73(6): 12991304.
Kretchmer, N. 1971. [Memorial lecture] Lactose and lactase: A historical perspective. Gastroenterology 61: 805-13.
1977. The geography and biology of lactose digestion and malabsorption. Postgraduate Medical Journal 53: 65-72.
Lebenthal1 E., et al. 1981. Recurrent abdominal pain and lactose absorption in children. Pediatrics 67: 828-32.
Quan, R., et al. 1990. Intestinal lactase: Shift in intracellular processing to altered, inactive species in the adult rat. Journal of Biological Chemistry 265: 15882-8.
Ransome-Kuti, O., et al. 1975. A genetic study of lactose digestion in Nigerian families. Gastroenterology 68: 431-6.
Sahi, T. 1974. The inheritance of selective adult-type lactose malabsorption. Scandinavian Journal of Gastroenterology (Supplement 30): 1—73.
Scrimshaw, N. S., and E. B. Murray. 1988. The acceptability of milk and milk products in populations with high prevalence of lactose intolerance. American Journal of Clinical Nutrition (Supplement 48(4)): 1083-1147.
Semenza, G., and S. Auricchio. 1989. Small-intestinal disaccharidases. In The metabolic basis of inherited disease, 6th edition, ed. C. R. Scriver et al. New York.
Simoons, F. J. 1970. Primary adult lactose intolerance and the milking habit: A problem in biologic and cultural interrelations. II. A culture-historical hypothesis. American Journal of Digestive Diseases 15: 695—710.
Sunshine, P., and N. Kretchmer. 1964. Intestinal disaccharidases: Absence in two species of sea lions. Science 144: 850-1.
Wald, A., et al. 1982. Lactose malabsorption in recurrent abdominal pain of childhood. Journal of Pediatrics 100: 65-8.
More on the topic 75 Lactose Intolerance and Malabsorption:
- 75 Lactose Intolerance and Malabsorption
- Contents
- Kiple Kenneth F. (Editor). The Cambridge World History of Human Disease. Cambridge University Press,1993. — 1200 p., 1993