81 Leptospirosis
The kind of leptospirosis manifested by severe jaundice was first described as a human disease in 1886 by A. Weil. Named Weil’s disease the following year, the term was meant to designate a distinctive infectious jaundice, and it would not be known until much later that leptospirosis was caused by numerous Ieptospires that triggered various clinical syndromes.
The first of the causative pathogens were independently discovered in 1915 by R. Inada among Japanese mine workers and by P. Uhlenhut and W. Fromme among German soldiers. Leptospira, a genus of the family Treponemataceae, order Spirochaetales, is a fine threadlike organism with hooked ends (see Figure VIII.81.1) that is pathogenic for humans and other mammals, producing meningitis, hepatitis, and nephritis both separately and together. In the past, the disease killed between 15 and 40 percent of those infected. Modern treatment has reduced mortality to about 5 percent. As a zoonosis, the disease is generally maintained in rodent reservoirs.Etiology and Epidemiology
Leptospires are obligate aerobes and classified serologically as a bacterium, subdivided into two species. One is Leptospira biflexa, which includes the various water spirochetes, whereas the other, Leptospira interrogans, embraces the parasitic strains. The species interrogans (so named because of an appearance like a question mark) is now subdivided by the main antigen into 187 serotypes or serovars. Human leptospirosis generally results from direct or indirect exposure to the urine of infected animals, although it can also be transmitted by handling infected animal tissue, by animal bites, and by the ingestion of contaminated food and water. The Ieptospires can enter the body through breaks in the skin, as well as through the lining of the mouth, nose, and eyes.
Persons of all ages are susceptible to the infection, and although the disease may occur at any time, it is most often seen during warmer weather and periods of heavy rainfall.
Its presence in mud and swamps has often placed soldiers at special risk. As a rule, it appears as isolated cases, but it can also manifest itself in small clusters and even in large outbreaks, depending on the type and the circumstances of its transmission.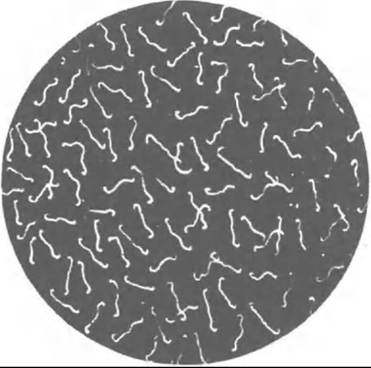
Figure VIII.81.1. Leptospires on dark field. (From O. Gsell. 1978. Leptospires and relapsing fever. In Handbook OfClinical Neurology, Part III, Chapter 18, 395418, by permission of Elsevier Science Publishing.)
In most of the world, leptospirosis is an occupational disease. Field workers and those who work around farm animals are at risk, as are employees of slaughter houses and poultry and fish production plants, and persons employed in sewers, mines, and in other wet places infested with rodents. Infected wild animals such as rats and mice are the source of infection for domesticated animals, especially dogs (Leptospira canicola), pigs (Leptospira pomona), and cattle (Leptospira hardjo), who may in turn infect humans.
As Table VIII.81.1 indicates, localized leptospirosis infections produced by one or another strain of the pathogen occur across the globe. The pig-raising areas of the European alpine region, northern Australia, and parts of Argentina see one form of the disease caused by L. pomona and Leptospira hyos or tarassoυi and called swineherd’s disease. Similarly, the sugarcane plantation regions of East Asia and rice-growing regions of Spain and Italy harbor other forms, which are the result of infection by field mice. Local names for the various forms of leptospirosis often reflect the circumstances under which it is contracted. Thus there is “harvest” or “swamp” fever, caused by Leptospira grippotyphosa. In Germany, agricultural workers contracted “field fever”; in Silesia, there was “mud fever”; in Russia, “water fever”; and in Germany and Switzerland, “pea pickers disease.” On the other hand, leptospirosis can also be an urban disease carried by the ubiquitous Rattus norwegicus, as well as by dogs.
Table VΠI.81.1. Serologic classification Ofleptospires
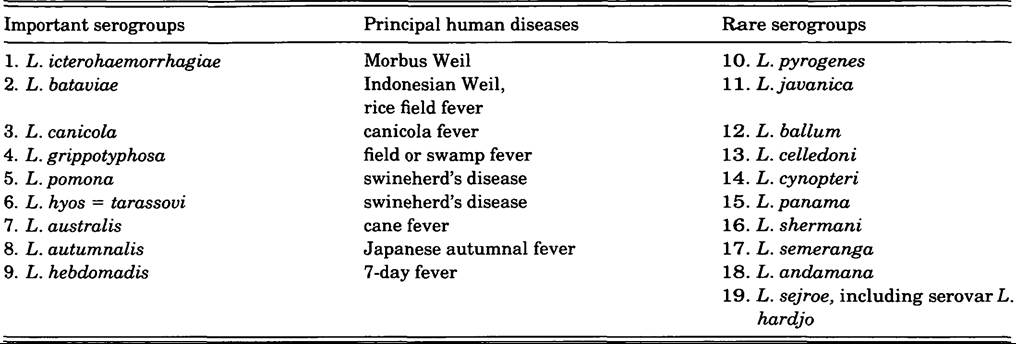
Source: 0. Gsell. 1978. Leptospiroses and relapsing fever. In Handbook of Clinical Neurology, Part III, Chapter 18, 397. New York: Elsevier Science Publishing, by permission of publisher.
Clinical Manifestations
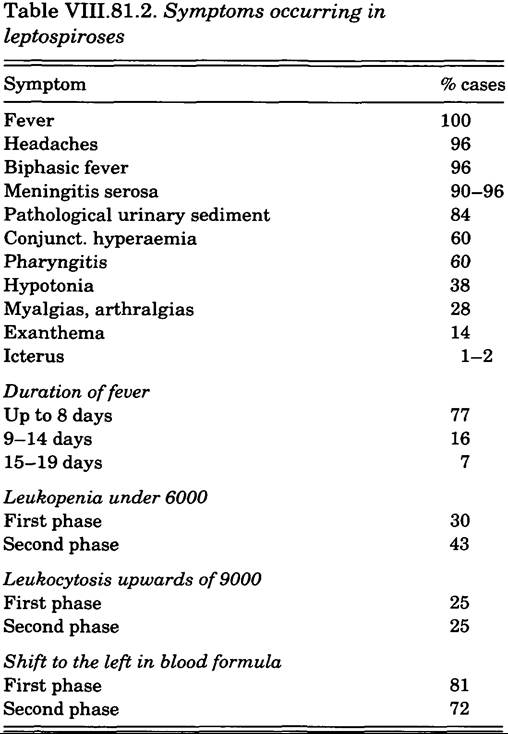
Figure VIII.81.2 shows the phases of leptospirosis and the relevant diagnostic procedures. The first phase of the disease is characterized by an acute onset of high fever, headache, malaise, conjunctival reddening, muscle pain, often meningism, renal irritation, hypotonia, and relative bradycardia (see Table VIII.81.2). In the second stage, there is danger of organ involvement, which is accompanied by the appearance of specific antibodies in the serum. The disease frequently causes the liver to become enlarged and painful, and can be life-threatening when renal damage is severe. Icterus, when it occurs, can be very intense and last for several weeks. Leptospirosis also causes kidney damage, although the most common second-stage symptom is serosal meningitis, and less frequently encephalomyelitis or neuritis. Swineherds’ meningitis is particularly well known (Gsell 1952). Meningitis symptoms usually subside completely in the third week.
As Figure VIII.81.2 indicates, there can be other damage from the disease, but only rarely. When it causes death, postmortem findings reveal renal and hepatic failure represented by renal tubular necroses, hemoglobinemia, and liver cell necrosis with general jaundice and anemia. Hemorrhages can be found in almost any organ, and in muscles and subcutaneous tissue.
Treatment
Antibiotics are quite effective against Ieptospires but only if employed within the first 3 or, at the most, 4 days. After this, efforts should be directed at avoiding complications. Severe kidney insufficiency requires hemodialysis or peritoneal dialysis, and infusions or transfusions may be necessary as well.
History and Geography
Much of the history of leptospirosis appears as an effort to separate leptospiral jaundice and meningitis from other infections. The clinical portion of this history began with Weil’s description of the disease in 1886; the bacteriologic phase began with isolation
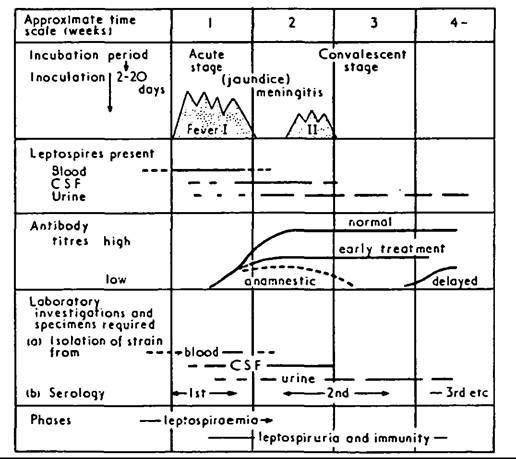
Figure VIII.81.2. Phases and relevant diagnostic procedures of leptospiroses. (Reproduced with slight modification from L. H. Turner 1973, in O. Gsell. 1978. Leptospiroses and relapsing fever. In Handbook of Clinical Neurology, Part III, Chapter 18, 395—419; 399, by permission of Elsevier Science Publishing.)
Source: 0. Gsell. 1978. Leptospiroses and relapsing fever. In Handbook of Clinical Neurology, Part III, Chapter 18, 399. New York: Elsevier Science Publishing, by permission of the publisher.
of the pathogenic germs in 1915 by Inada and Uhlenhut and Fromme. In 1918, H. Noguchi gave the name Leptospira to the newly discovered bacteria. During the years 1917—18 Y. Indo, H. Ito, and H. Wani found cases of the disease that were not characterized by jaundice — described as the 7-day fever “Nanukayami” which has the field mouse as a carrier. In the following decades, numerous different serotypes were found throughout the world. Among these are Leptospira pyrogenes (Indonesia, 1923), Leptospira autumnalis (Japan, 1925), Leptospira ba- taviae (Indonesia, 1926), L. grippotyphosa (Russia, 1928), Leptospira andaman (Andaman Islands, 1931), L. canicola (Netherlands, 1933), Leptospira australis as well as L. pomona (Australia, 1937), and Leptospira hebdomadis hardjo (Great Britain, 1968).
In Switzerland during the year 1944, L. pomona was found to be the cause of swineherds disease with the pig as its carrier, and 4 years later L. tarassovi and L. hyos were discovered to be of the same serotype and also carried by the pig.
Numerous other serovars have been discovered subsequently, and after 1950 a new classification of the serotypes was accepted which classified the clinical groups into malignant and benign human Ieptospires, while in serology it permitted the allocation of animal and human Ieptospires to different serovars. In looking back on a century of research on leptospirosis, it seems remarkable that serious and widespread epidemics have been so infrequent. Today the incidence of the disease has been reduced in developed countries, probably because of a decrease in the rodent populations and because of improved human hygiene in the presence of domestic animals.OttoR. Gsell
Bibliography
Alston, J. M., and J. C. Broom. 1958. Leptospiroses in man and animal. London.
Faine, S. 1982. Guidelines for the control Ofleptospirosis. World Health Organization Offset Publication No. 67. Gsell, O. 1952. Leptospirosen. In Handbuch der Inneren Medizen, 4th edition, 21-45. Berlin.
1974. Leptospirosen. Klinik der Gegenwart, Vol. 2, ed. H. E. Bock, W. Gerock, and F. Hartmann. Miinchen.
1978. Leptospiroses and relapsing fever. In Handbook of Clinical Neurology, Part III: 395-419. New York.
1984. History of leptospiroses: IOO years. Zentralblatt fur Bakteriologie und Hygiene A257: 473-8.
1990. Leptospiroses. Zentralblatt fur Bakteriologie und Hygiene 281: 109-26.
Symposium of the leptospiroses, December 1952. 1953. Washington, D.C.
Turner, L. H. 1973. Leptospiroses III. British Medical Journal 1: 537-40.