80 Leprosy
Leprosy occurs naturally only in humans and is caused by infection with Mycobacterium leprae. Known also in the twentieth century as “Hansen’s disease,” after the Norwegian microbiologist A.
G. H. Hansen who first isolated the microorganism in 1873, true leprosy is a chronic, debilitating, and disfiguring infection. However, the long history of disease attributed to leprosy undoubtedly includes a broad range of skin and systemic afflictions that only resembled leprosy symptoms.The leprosy bacillus multiplies quite slowly, usually in the sheaths of peripheral nerves. Losing sensation in discrete, patchy areas of the skin is often the earliest, but ignored, symptom of infection. Lacking adequate innervation, the affected dermis can be damaged without evoking a pain response as, for example, by a burn or a cut. Repair of the tissue is then hindered by poor regulation of local blood supply. Hence, secondary infection and inflammation of an involved area are common, leading to scarring and callusing of surviving tissues. This long process can result in the loss of fingers, toes, nasal tissue, or other parts of the body frequently exposed to the elements. A “bear claw” foot or hand becomes one of the characteristically maiming and stigmatizing features of the leper. Involvement of the nasal cartilage and vocal cords, common sites for the organism’s growth, leads to profound disfiguration of the center of the face and also to the raspy, honking voice described in some historical accounts of true leprosy.
The early and more subtle physiological changes caused by leprosy have been noted consistently only since the nineteenth century. Owing to the involvement of nerves supplying the dermis, the heavily innervated face loses “free play” of expression and affect. Eyelashes and the lateral part of the eyebrows disappear long before other, grosser signs betray infection.
Distribution and Incidence
In the late twentieth century, leprosy occurs commonly only in tropical and subtropical regions, as indicated in Map VIII.80.1. There are at least 15 million lepers worldwide, most of them residing in Africa, South and Southeast Asia, and South America. However, this geographic distribution of the disease more likely reflects the poverty of these regions than it does the possibility that elevated temperatures and humidity facilitate infection. Despite cheap and effective medication (dapsone) to arrest the relentless progression of leprosy in infected individuals, the disease continues to spread in the rural regions of Africa, Southeast Asia, and the Indian subcontinent. Often because leprosy stigmatizes its victims socially, leading to loss of employment, alienation from family and community, and, ultimately, to confinement in a leprosarium, lepers deny infection or evade treatment as long as they can. In the process they ensure transmission of the disease to others. Leprosy is normally passed from one individual to another only with sustained exposure, but the disease continues to spread even in areas served by Western medical practitioners, because of the high social costs of early identification and treatment.
In the past, leprosy probably extended as far north as the Arctic Circle. Extensive paleopathological investigations of medieval gravesites thought to have belonged to leper colonies have produced evidence of leprosy among Danes and Norwegians of the thirteenth century. Interestingly, the distribution of leprosy in medieval Europe, like that of today, appears to have been rural, and the written or physical evidence of leprosy disappears with urbanization. The disappearance of leprosy in Europe historically progressed gradually northward from the urban Mediterranean areas of Italy and Spain. Cases of leprosy were still reported in England and Scotland during
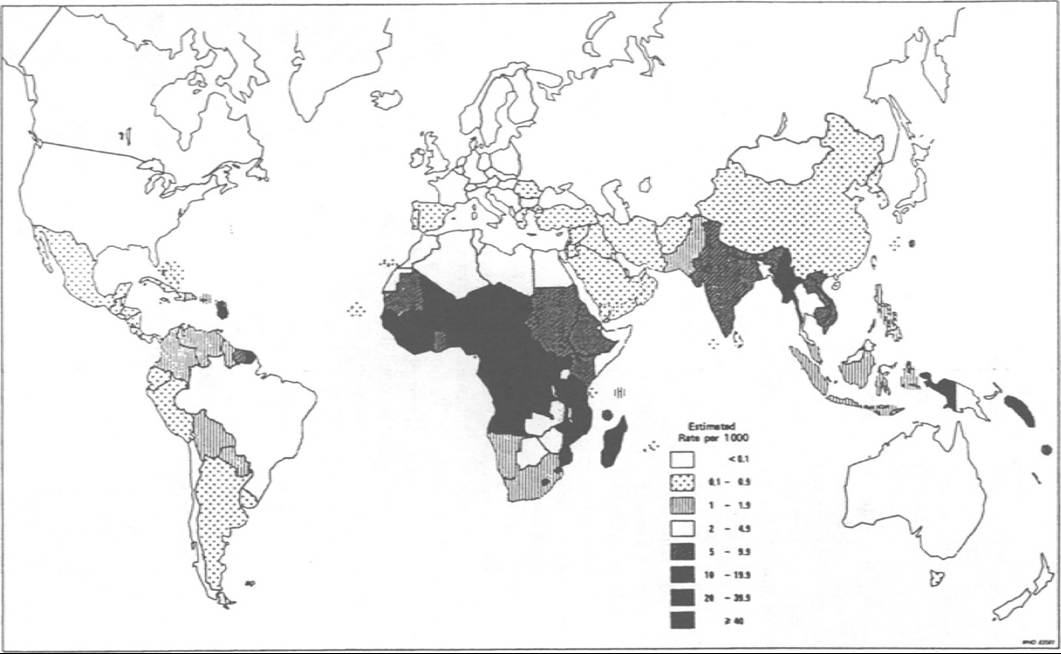
Map VIΠ.80.1.
Estimated endemicity of leprosy in the world, 1983. (From World Health Organization. 1985. Epidemiology of leprosy in relation to control: Report of a WHO Study Group. World Health Organization Technical Report Series 716. Geneva.)Cambridge Histories Online Cambridge University Press, 2008
the fourteenth and fifteenth centuries, and the disease persisted in Scandinavia until the late nineteenth century, where Hansen discovered the bacillus that causes the disease.
One of the odd features of the geographic distribution of leprosy is the increased prevalence on islands or near seacoasts. Late medieval and early modem theorists even attributed the cause of the disease to an exclusively fish diet, an explanation now discredited. Undoubtedly the low infectivity of the disease and its association with poverty and poor sanitation contribute to the slow spread inland once leprosy is introduced into a region.
Epidemiology
It is possible that the history of Mycobacterium tuberculosis, an organism related to leprosy and one that creates a limited cross-immunity to M. leprae infection, has affected the long-term distribution and incidence of leprosy, as may also have other atypical mycobacterial infections such as scrofula and avian tuberculosis. Increased population density in urban areas facilitates the spread of tuberculosis infection, which may have contributed to a declining incidence ofleprosy as cities and large towns appeared. In large regions of West Africa today, leprosy’s hold over rural, remote villages increases with distance from a city (Hunter and Thomas 1984), whereas tuberculosis infection, evidenced by positive reactions to a tine or tuberculin purified protein derivative (PPD) test, increases dramatically with population density. There is almost no evidence that leprosy existed in the Western Hemisphere, Australia, or Oceanic Islands before it was introduced from the Old World.
This epidemiological relationship between tuberculosis and leprosy, however, is obscured in individual patients.
For despite cross-immunity, the most common associated cause of death in leprosaria is tuberculosis, illustrating how long-sufferers of leprosy lose the ability to combat other chronic infections. Moreover, geographic determinants of leprosy infection alone cannot explain the high prevalence of leprosy in densely settled eastern India. It could be, however, that more successful control of tuberculosis in the region permitted the persistence of leprosy and that stigmatization of lepers effectively delayed treatment of the illness by medical and public health authorities.Etiology
M. leprae belongs to a large group of intracellular bacterial pathogens widely distributed in nature. Members of the family Mycobacteriaceae can infect mammalian and avian hosts, and, as exemplified by bovine tuberculosis and avian tuberculosis, a pathogen dominant in one host species can successfully infect an altogether different host. Thus humans have suffered from bovine tuberculosis transmitted through contaminated cow’s milk and from atypical mycobacterial infections in the form of “scrofula” or infected lymphatic glands. But among these, only leprosy and tuberculosis can be successfully transmitted from one human to another, although M. leprae is the only one of these genera that cannot be transmitted naturally to species other than humans.
This feature of leprosy made difficult the search for a suitable experimental animal for research, and only during the mid-1960s did medical scientists succeed in transmitting the infection to armadillos of the American Southwest. In what period of human history M. leprae appeared, and from what other mycobacterial species it evolved are a mystery. Paleopathological evidence confirms the existence of true leprosy in the ancient eastern Mediterranean basin. It was probably African in origin and steadily disseminated among human communities from Pleistocene times onward (Grmek 1983).
The organism usually enters a new human host through respiratory passages or the skin.
Because the period of incubation (i.e., the interval between infection and the manifestation of symptoms) is so long, the actual process of the microorganism’s growth and dissemination through the body is not well understood. Commonly, early symptoms of disease appear 3 to 5 years after infection, but clinical evidence of infection may appear in as little as 6 months, or as long as 20 years post infection.Clinical Manifestations and Pathology
Typically leprosy first appears on the skin as a patch or area thickened and differing in color from the Sinrounding skin. It may be darker or lighter in color, but is usually distinguishable because the area is unresponsive to touch or pain. As is true of other chronic infectious diseases, such as tuberculosis, syphilis, or acquired immune deficiency syndrome, the clinical features of leprosy can vary from one sufferer to another. Leprosy is in fact described as a “bipolar” disease because of two very different clinical forms of the illness, with “mixed” or “indeterminate” reactions to infection possible but less frequent. The intermediate type is sometimes called “borderline” as well. Individuals whose clinical course vacillates between the two polar types are also viewed as intermediate.
In tuberculoid leprosy, one of the polar types, the areas of “patchy anesthesia” on the skin heal relatively quickly after injury, but new areas appear, more extensive and severe, and the untreated disease involves peripheral nerves to such an extent that desensitized skin cannot be protected from bums, exposure, or other insults to the body surface. Even though tuberculoid leprosy is thought to be milder than Iepromatous leprosy, possibly because of a stronger immune response to infection, the secondary infections after skin injury make it a serious disease.
In the “leonine facies” of Iepromatous leprosy, the other polar type, the reaction on the skin surface is dramatic and severely disfiguring, because the intermediate healing of involved skin produces thick, corrugated scar tissue.
The lesions are often teeming with infective bacilli. The two clinical forms are not caused by morphologically distinguishable forms of M. leprae. Thus either a strong or a weak immunologic response (if this difference is the “cause” of the two forms of disease) produces crippling and disfigurement.The leonine form is more distinctive by sight and thus is more frequent in historical accounts closely describing leprosy. Chinese surgeon Hua T’o’s description (around A.D. 150) is a good one:
The skin is first numb without sensation, gradually red spots appear on it, when it is swollen and ulcerated without any pus. And later the disease develops to such an extent that the eyebrows fall, the eyes may become blind, the lips deformed and the voice hoarse. The patient may also experience ringing in his ears and the soles of his feet develop rotted holes; his finger joints may become dislocated and the bridge of his nose flattened. (Skisnes 1973)
On the other hand, exaggerated, grossly disfiguring ulceration of face and limbs is not necessarily caused by leprosy. Syphilis, repeated frostbite injury, and diabetes could also account for the features given in this eighteenth-century Japanese description:
[I]t is useless to attempt to cure a patient whose eyes have a yellow hue [a reflection of either liver damage or the destruction of red blood cells], whose fingernails have no white crescents at the bottom, whose hands are wholly anesthetic, whose palm or sole bleeds, whose eyeballs are ulcerated, whose penis is putrified, whose hands or feet are clawed, whose skin is spotted with black, whose fingers have melted off leaving frog-foot shaped ends, whose body hairs fall off, whose nose is gone, whose bones are poisoned and putrified. (Skisnes 1973)
In addition, secondary infection by many nonin- fectious diseases such as psoriasis, pellagra, eczema, and lupus erythematosis could easily have led to this historical diagnosis of leprosy. Thus the more subtle changes of early leprosy, such as the loss of the lateral third of the eyebrows, the hoarse voice, the areas of patchy anesthesia, and the loss of free play in facial musculature - all features of the diagnostic procedure described by tenth-century Persian physician Avicenna - provide more assurance of a correct diagnosis of leprosy than does simply Ioathesome appearance.
Untreated, the established leprosy infection today usually progresses slowly, although there are periods of rapid worsening in a person’s overall ability to contain the disease. During these periods of exacerbation, severe pain can be caused by involvement of the nerves, and nodules on the skin may appear rapidly and in crops of lesions. It is rare to die, however, from unchecked Hansen’s disease; secondary infection usually leads to the patient’s demise.
Immunology
Because leprosy is caused by an intracellular pathogen, production of circulating humoral antibodies (the immunoglobulins) is of little use in combatting the infection of cells and the multiplication of the organism in human tissues. Cell-mediated, or T-cell, immunity is thus the principal bodily means of combating leprosy. Individuals in whom the expression of cell-mediated immunity is compromised or poorly developed, such as pregnant women and children younger than 2 years of age, are at greater risk for both infection (when initially exposed) and progression of the disease unimpeded by the immune system. Others with intact cellular immunity can live almost 20 years before the first serious, debilitating consequences of infection occur. It is not known to what extent recurrent viral infection, which also challenges cellular immunity, may hasten the onset of clinical leprosy.
Genetic factors may further mediate the clinical expression of leprosy among those already infected, predisposing some individuals to a more or less rapid course of the disease, or perhaps influencing the appearance of severe, Iepromatous leprosy rather than the milder tuberculoid form. Nevertheless, there are only a limited number of cases in which some clear genetic determinant of susceptibility can be differentiated from the socioeconomic factors mediating exposure to the agent.
History and Geography
The history of leprosy has been dominated by three questions or problems. One question concerns stigmatization. Most ancient societies identified some individuals as “lepers,” and the leper was stigmatized, although surely lepers as a group included many suffering from something besides Hansen’s disease. Stigmatization of the leper has persisted into the late twentieth century despite advances and refinements in the medical diagnosis and treatment of leprosy. The second problem focuses on medical evidence for leprosy’s changing incidence and prevalence over time, particularly in western European history during the period between 500 and 1500 of the present era. Finally, the world distribution of leprosy and failures to impede its spread have emerged as a historical problem of the past 250 years.
In the Old Testament Book of Leviticus, the disease zara’ath or tsara’ath was identified by priests and its victims were cast “outside the camp” as unclean and uncleansable. They were viewed as both chosen and rejected by God and, consequently, not exiled altogether from the community, as were criminals, but rather made to live apart as if the living dead. Thus, central problems posed by the disease zara’ath involved, on the one hand, the spiritual identity of diseased individuals who, although probably morally “tainted,” were not, apparently, personally responsible for their disease; and on the other hand, the delegation of the process of making the diagnosis to religious, not medical, authorities.
Because the opprobrium attached to leprosy was handled dramatically by writers of the Biblical Old Testament and because this Judaeo-Christian tradition was of central importance to western European history for the next 2,000 years, stigmatization of the leper was derived from religious, medical, and social responses to individuals carrying the diagnosis. Thus, during the High Middle Ages (A.D. 11001300), lepers were identified by priests or other spiritual authorities, and then separated from the general community, often Htualistically. Considered “dead to society,” last rites and services might be said in the leper’s presence, sometimes as the victim stood symbolically in a grave. Thereafter the person’s access to his or her city or village was severely limited. Italian cities, for example, posted guards at the city gates to identify lepers and deny them entrance except under carefully controlled circumstances. Leprosaria, or isolation hospitals to house lepers, were constructed at church or communal expense, although medical services to these facilities were limited. Where public services were less well organized, lepers had to depend upon begging or alms.
Laws in western Europe illustrated the exaggerated fear of contagion lepers generated. Lepers had to be identifiable at a distance, leading to the creation of legendary symbols of the leper: a yellow cross sewn to their cape or vestment; a clapper or bell to warn those who might pass by too closely; a long pole in order to point to items they wished to purchase, or to retrieve an alms cup placed closer to a road than lepers were allowed to go.
The stigmatization of lepers, however, was not limited to Western tradition, and in most societies of the past those labeled as lepers were denied legal rights in addition to being socially ostracized. In traditions of both East Asia and the Indian subcontinent, marriage to a leper or the offspring of a leper was prohibited, and, as in Western tradition, the disease was often attributed to moral causes (sin) as well as to contagion. Interesting in this regard is the monographic representation of the leper in Tibetan art, a man covered with vesicles and ulcers, which parallels Western depictions of Job as a man covered by sores in punishment by God for his sins. The stereotype of the leper as filthy, rotten, nauseating, and repulsive is so strong that most “hansenolo- gists” today advocate rejection of the name “leprosy” in favor of Hansen’s disease. The only exception to this pattern of stigmatization seems to be in Islamic society, where the leper is neither exiled nor considered perverse, promiscuous, or otherwise morally repulsive (Dols 1983).
In contrast to ancient Chinese texts of approximately the same period, in which leprosy destroying the center of the face is well described, the clinical evidence for leprosy in the ancient Mediterranean is meager. Nowhere in the Biblical tradition is there more than a general description of the disease that created such a severe response. Hippocratic texts provide no evidence that true leprosy existed in ancient Greece, but the Hippocratic, Greek word lepra, probably describing psoriasis, gave origin to the disease’s name. Thus a coherent and powerful tradition in the West stigmatizing the leper was begun in what appears to have been the absence of any organized and reasonably accurate medical description of how these sufferers could be identified. Indeed, the earliest clinical description of leprosy in the West appears neither in the Hippocratic corpus (written in Greek between 400 and 100 B.C.) nor in the 20 surviving volumes of the works of the great second- century Greek physician, Galen, but rather in the writings of the tenth-century Persian physician Avicenna, and it is his Canon OfMedicine that provides the description upon which medieval European physicians relied.
The decline of leprosy in Europe coincided with increasing medical sophistication in diagnosing what we might recognize as leprosy. This decline may be due in part to an increase in another mycobacterial disease such as tuberculosis; to improvements in living standards; to high catastrophic mortality from plague and other epidemics, effectively reducing the number of lepers in the general population; or to the simple fact that medical authorities began to share the burden of diagnosis with religious and communal leaders. Surely other skin infections and afflictions that might earlier have been taken for leprosy were better recognized in the late Middle Ages. Nonetheless true leprosy certainly existed in Europe, as the exhumations of medieval skeletal materials from northern Europe have well illustrated (M011er- Christensen 1961; Andersen 1969; Steinbock 1976).
Knowledge of leprosy in modem medical terms evolved during the nineteenth century, coincident with development of the germ theory of disease. During this period, the precise description of the clinical characteristics Oflepromatous leprosy by Danish physician Daniel C. Danielssen in the 1840s; the discovery of the microorganism by Hansen in 1873; and widespread attention to the contemporary geographic distribution of leprosy in European colonial territories served to identify the disease as a contagious tropical infection. As such it was believed to be eradicate by Western medical efforts in public health intervention. Methods of quarantine and isolation were enthusiastically employed, despite skepticism about these methods in general public health control.
In the same year that Hansen found the causal organism of leprosy, a devoted Catholic priest, Father Damien de Veuster, drew worldwide attention in an attempt to humanize the treatment of leprosy by going to live among lepers in Hawaii. But he may have underscored fear of the contagion of leprosy because he eventually contracted the disease. Thus in modem times, increasing medical knowledge of the incidence and prevalence of M. leprae may have served to increase alarm and fear as leprosy was “discovered” to be the resilient global problem it remains to this day.
Ann G. Carmichael
Bibliography
Andersen, J. G. 1969. Studies in the mediaeval diagnosis of leprosy in Denmark. Danish Medical Bulletin (Supplement) 16:1—142.
Brody, Saul Nathanial. 1974. The disease of the soul: A study in the moral association of leprosy in medieval literature. Ithaca.
Clay, Rotha Mary. 1909. The medieval hospitals of England. London.
Clark, George A., et al. 1987. The evolution of mycobacterial disease in human populations: A reevaluation. Current Anthropology 28: 45—62.
Demaitre, Luke. 1985. The description and diagnosis of leprosy by fourteenth-century physicians. Bulletin of the History OfMedicine 59: 327-44.
Dols, Michael W. 1983. The leper in medieval Islamic society. Speculum 4: 891-916.
Ell, Stephen R. 1984. Blood and sexuality in medieval leprosy. Janus 71:153-64.
Grmek, Mirko D. 1983. Les Maladies a Vaube de la civilisation occidentale: Recherches sur la realite patho- Iogique dans Ie monde grec prehistorique, archa'ique et classique. Paris.
Grδn, K. 1973. Leprosy in literature and art. International Journal of Leprosy 41: 249—83.
Gussow, Z., and G. S. Tracy. 1970. Stigma and the leprosy phenomenon: The social history of a disease in the nineteenth and twentieth centuries. Bulletin of the History OfMedicine 44: 425—49. ∙
Hunter, John M., and Morris O. Thomas. 1984. Hypothesis of leprosy, tuberculosis, and urbanization in Africa. Social Science and Medicine 19: 26—57.
Mpller-Christensen, V. 1961. Bone changes in leprosy. Copenhagen.
Palmer, Richard J. 1982. The church, leprosy and plague in Medieval and Early Modem Europe. In The church and healing: Studies in church history, No. 19. ed. W. J. Shields. Oxford.
Richards, Peter. 1977. The medieval leper and his northern heirs. Cambridge.
1971. Leprosy in Tibetan art and religion. International Journal of Leprosy 39: 60—65.
Skisnes, Olaf K. 1973. Notes from the history of leprosy. International Journal of Leprosy 41: 220-37.
Steinbock, R. T. 1976. Paleopathological diagnosis and interpretation. Springfield, Ill.
World Health Organization. 1985. Epidemiology of leprosy in relation to control: Report of a WHO Study Group. Technical report series 716. Geneva.