86 Marburg Virus Disease
History
In 1967, a disease outbreak occurred in a laboratory in Marburg, Germany, where the kidneys of Cercopithecoid (Green African; vervet) monkeys were being taken out for preparation of cell cultures.
Twenty-seven laboratory workers (including a worker in Yugoslavia) fell ill with a grave illness, and seven died. There were four secondary cases in total (including the wife of an infected laboratory worker in Yugoslavia secondarily infected by sexual intercourse), but none fatal. Early suspicions focused on yellow fever, but this was soon ruled out (Casals 1971). In due course, a virus was isolated and found to be quite distinct from any other known viruses. Electron micrographs revealed a virus with bizarre morphology of a type never seen before (Peters, Muller, and Slenckza 1971). Pictures taken resembled photographs of a bowl of spaghetti. The agent was named Marburg virus and the disease Marburg disease. Strict monkey quarantines were initiated. No further cases were seen in laboratory workers.An intensive and extensive series of field studies were initiated in East Africa, which had been the monkeys’ homeland (Henderson et al. 1971; Hennes- sen 1971; Kalter 1971). No virus recoveries were made from any of the monkeys examined. In later years, serologic studies involving humans and primates, and also rodents, have been carried out in many regions, as can be seen in Table VIII.86.1.
The first Marburg cases seen in Africa occurred in February of 1975. A young Australian couple touring in Rhodesia (Zimbabwe) became ill by the time they got to South Africa. They were admitted to a major hospital in Johannesburg where the young man died and the young lady recovered. A nurse tending them also sickened and recovered. After the disease was determined to be Marburg, a thorough epidemiological inquest was carried out all along the
Table VIΠ.86.1.
Serologic studies of Marburg virus in humans and other primates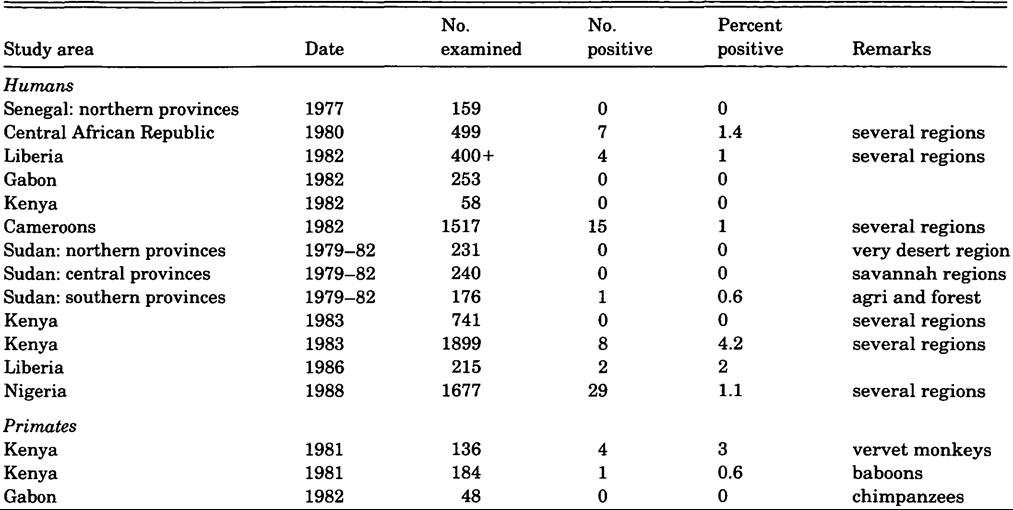
route of passage of the victims, concentrating particular attention on every locale where they spent a night. Animal, insect, and human populations were sampled. No evidence of endemic disease was found (Gear et al. 1975).
On January 14,1980, a 58-year-old man from western Kenya was seen in a Nairobi hospital. He died 6 hours after admission, and a physician who attended him also became ill but recovered. A Marburg virus was isolated from his blood (Centers for Disease Control 1980). Subsequent epidemiological investigations carried on in western Kenya produced a positive finding: Antibodies against the Marburg virus were found in two vervet monkeys from among many primates examined.
The latest episode involved a boy in Kenya in 1987 who became infected in a visit to a park in the western part of Kenya. The boy died. There were no secondary cases reported.
Etiology
Electron microscopic examination of blood, liver, and spleen of guinea pigs infected with materials from patients show a long, viruslike agent, quite unlike any virus particle ever before visualized. The particles vary in length, up to several microns. The width of the particles is also variable, with limits of 720 to 1100 A (7,200 to 11,000 nanometers). There is an outer shell, an intermediate clear zone, and a nucleo- capsid core of approximately 280 A width (Peters et al. 1971). Marburg virus was shown (Casals 1971) to be unrelated to the many arboviruses against which it was tested, and most closely resembles the Ebola virus agent discovered in 1976. In fact, both Marburg and Ebola viruses have since been placed in a new family, Filoviridae (Kiley et al. 1982), which includes but the two members thus far.
It was discovered that the Marburg virus could be inactivated by gamma irradiation (Elliot, McCormick, and Johnson 1982); this finding made the preparation of inactivated diagnostic reagents possible.
Cultivation of Marburg in cell culture has allowed observation of growth and multiplication taking place in a number of mammalian and avian cell types. A Cytopathic effect on cells was observed in Cercopithecus kidney cell lines, and human amnion cell lines (Hoffmann and Kunz 1971).Immunoglobulin responses have been studied (Wulff and Johnson 1979), measured by immunofluorescence. Immunoglobulin M antibodies appear in sera of patients infected with Marburg virus 4 to 7 days after onset of illness. Titers peak 1 to 2 weeks later, and by 1 to 2 months have decreased considerably. Antiviral IgG antibodies appear at the same time as or a little later than IgM antibodies and persist much longer (Wulff and Johnson 1979). In autopsy material, antigenic material is present in large amounts, and can be demonstrated as late as 3 hours after death by use of Immunofluorescent techniques (Wulff, Slenczka, and Gear 1978).
Clinical Manifestations and Diagnosis
The incubation period following exposure varied from 5 to 7 days. In six cases for which data are available, death occurred between days 7 and 16. The onset was indicated by malaise, myalgia, and often prostration (Martini 1971). Vomiting frequently occurred by the third day, and conjunctivitis by the fourth, by which time the temperature had reached 40oC. A rash occurred on the fifth day, was macular in type, and progressed usually to a maculopapular rash that later coalesced into a more diffuse rash. In severe cases, a diffuse dark livid erythema developed on face, trunk, and extremities. An enanthem of the soft palate developed at the same time as the rash. Spleen and liver were not palpable. Lymph node enlargement was noted in the nuchal region and the axillae. A diarrhea appeared, often with blood in the stools. The South African cases differed only in that there were no enanthem and no lymph node enlargement.
The above description was declared by several clinicians to make diagnosis easy.
This may be true when there is a clustering of cases, and epidemiologists are on the alert; however, in much of Africa, the occurrence of single cases, however severe, would not be likely to arouse suspicion. Moreover, during the first 5 to 6 days, the symptoms could be mistaken for those of many other diseases. Laboratory diagnosis is accomplished by means of immunofluorescence techniques, by electron microscopic examination of a serum sample from a patient, which has been centrifuged and placed on a grid (Wulff et al. 1978), and by inoculation of laboratory animals. None of these methods is readily accessible in the usual field situation; yet early diagnosis is imperative in order to abort a possible developing epidemic.Mortality
Because descriptions of Marburg virus pathology are equally applicable to Ebola virus, some pathologists feel that the findings are not distinctive enough to permit a positive diagnosis of either on the basis of pathology alone, especially in regions where there are many causes of fever and death.
Guinea pigs and rhesus and vervet monkeys are susceptible to the virus. The infection is fatal for the monkeys and, often but not always, fatal for the guinea pigs. Guinea pigs that recover may have persistent virus in serum and urine for several weeks. The same has been observed for human beings.
Ebola virus infection is considerably more fatal in humans than is the Marburg virus. In the four secondary Marburg cases studied, it was clear that their clinical course was less severe than that seen in primary cases, and there was no mortality.
Treatment and Prophylaxis
No effective therapy has been found. In one case in a London treatment center, therapy was instituted using interferon in conjunction with immune plasma. The patient, a secondary exposure case, recovered. Further clinical trials on human beings await further cases.
Basic methods for the management of patients with suspected viral hemorrhagic fever include strict isolation and precaution in examination and in taking specimens from patients, as well as in handling material from suspect cases in the laboratory.
Such procedures are not readily applicable in bush clinics in many parts of Africa. Further precautions are necessary in the movement of suspected cases internationally and in the shipment of specimens internationally (Simpson 1977; Centers for Disease Control 1988).Prophylaxis and control await further epidemiological information on animal reservoirs of disease, modes of transmission from animal reservoirs (if indeed there are animal reservoirs) to humans, and modes of persistence of the virus in nature.
Wilbur G. Downs
Bibliography
Casals, J. 1971. Absence of a serological relationship between the Marburg virus and some arboviruses. In Marburg virus disease, ed. G. A. Martini and R. Siegert, 98-104. New York.
Elliot, L. H., J. B. McCormick, and K. M. Johnson. 1982. Inactivation of Lassa, Marburg and Ebola viruses by gamma irradiation. Journal of Clinical Microbiology 16: 704-8.
Evans, A. S., ed. 1978. Viral infections of humans: Epidemiology and control, 2d edition. New York.
Fields, B. N., ed. 1985. Virology. New York.
Gear, J. H. S. 1988. CRC handbook of viral and rickettsial fevers. Boca Raton, Fla.
Gear, J. H. S., et al. 1975. Outbreak of Marburg virus disease in Johannesburg. British Medical Journal, November 29: 489-93.
Haas, R., and G. Maass. 1971. Experimental infection of monkeys with the Marburg virus. In Marburg virus disease, ed. G. A. Martini and R. Siegert, 136-43. New York.
Henderson, B. E., et al. 1971. Epidemiological studies in Uganda relating to the “Marburg” agent. In Marburg virus disease, ed. G. A. Martini and R. Siegert, 166— 76. New York.
Hennessen, W. 1971. Epidemiology of Marburg virus disease. In Marburg virus disease, ed. G. A. Martini and R. Siegert, 161-5. New York.
Hoffmann, H., and C. Kunz. 1971. Cultivation of the Marburg virus (Rhabdovirus simiae) in cell cultures. In Marburg virus disease, ed. G. A. Martini and R. Siegert, 112-16. New York.
Isaacson, M. 1988. Marburg and Ebola virus infections.
In CRC handbook of viral and rickettsial fevers, ed. J. H. S. Gear, 185-97. Boca Raton, Fla.Johnson, K. M. 1978. African hemorrhagic fevers due to Marburg and Ebola viruses. In Viral infections of humans: Epidemiology and control, ed. A. S. Evans, 95103. New York.
Kalter, S. S. 1971. A serological survey of primate sera for antibody to the Marburg virus. In Marburg virus disease, ed. G. A. Martini and R. Siegert, 177-87. New York.
Kiley, M. P., et al. 1982. Filoviridae: A taxonomic home for Marburg and Ebola viruses? Intervirology 18: 24-32.
Martini, G. A. 1971. Marburg virus disease, clinical syndrome. In Marburg virus disease, ed. G. A. Martini and R. Siegert, 1—9. New York.
Murphy, F. M. 1985. Marburg and Ebola viruses. In Virology, ed. B. N. Fields, Chapter 47. New York..
Peters D., G. Muller, and W. Slenckza. 1971. Morphology, development and classification of the Marburg virus. In Marburg virus disease, ed. G. A. Martini and R. Siegert, 68-83. New York.
Siegert, R., and W. Slenckza. 1971. Laboratory diagnosis and pathogenesis. In Marburg virus disease, ed. G. A. Martini and R. Siegert, 157-60. New York.
Siegert, R., H.-L. Shu, and W. Slenczka. 1968. Zur Diagnostic und Pathogenese der Infektion mit Marburg-virus. Hygiene Institut of Philipps University (Marburg University) MarburgILahn: 1827-30.
Simpson, D. I. H. 1977. Marburg andEbola virus infections: A guide for their diagnosis, management and control. WHO Offset Publication No. 36, Geneva. 1-28.
U.S. Public Health Service. Centers for Disease Control. 1988. Management of patients with suspected viral hemorrhagic fever. Morbidity and Mortality Weekly Report 37 (Feb. 26): 1-15.
Wulff, H., and K. M. Johnson. 1979. Immunoglobulin M and G responses measured by immunofluorescence in patients with Lassa or Marburg infections. Bulletin of the WorldHealth Organization 57: 631-5.
Wulff, H., W. Slenczka, and J. S. S. Gear. 1978. Early detection of antigen and estimation of virus yield in specimens from patients with Marburg virus disease. Bulletin of the World Health Organization 56: 633-9.