Nature of the Tobacco Hazard
Addictive Pleasures
Although it has always been obvious that tobacco contains a substance (nicotine) that yields psychic Table III.8.3. Percentage of U.S. adults who smoked regularly, 1945—85
| Year | Men (%) | Women (%) | Combined (%) |
| 48 | 36 | 42 | |
| 1950 | 54 | 33 | 44 |
| 1955 | 54 | 25 | 40 |
| 1960 | 52 | 34 | 42 |
| 1965 | 52 | 34 | 42 |
| 1970 | 44 | 31 | 38 |
| 1975 | 42 | 32 | 37 |
| 1980 | 38 | 30 | 34 |
| 1985 | 33 | 28 | 30 |
| 40-year | 46 | 31 | 39 |
| average |
Source: Estimated from survey data by Gallup Poll, National Center for Health Statistics, and Centers for Disease Control.
pleasures not obtained by the smoking of other plant leaves, only during the 1980s did a strong scientific and societal consensus emerge that nicotine is truly addictive - just as addictive as heroin or cocaine and much more addictive than alcohol.
Indeed, cigarette smoking is now the most serious and widespread form of addiction in the world. The proportion of adult men and women who have smoked cigarettes in the United States during the past halfcentury is indicated in Table III.8.3. Halfofadult men smoked at midcentury, this proportion decreasing to 33 percent in 1985 and 30 percent in 1987. Likewise, smoking by adult women decreased from 34 percent in 1965 to 28 percent in 1985 and 27 percent in 1987.
Lethal Poisons
The smoke of burning tobacco contains several thousand chemicals and a number of radioisotopes, including hydrogen cyanide, nitriles, aldehydes, ketones, nicotine, carbon monoxide, benzopyrenes, aza-arenes, and polonium 210, an alpha-particle emitter and therefore the most powerful contact mutagen, more than 100 times more mutagenic than equivalent RADs of gamma radiation. The combination of an addictive substance (nicotine) and more than 50 potent mutagens (especially polonium 210) has made tobacco the foremost human poison of the twentieth century.
Pathogenic Mechanisms
When tobacco smoke is inhaled deeply into the lungs, most of the tars contained therein are captured and retained by the respiratory mucous blanket. Soluble components are then promptly absorbed into the pulmonary circulation and conveyed by the systemic circulation throughout the body. Less soluble tars trapped by the mucous blanket are raised by ciliary action and coughing to the pharynx, then swallowed; thereafter, they pass to the esophagus, stomach, small intestine, portal circulation, and liver. Hence, chronic inhalation of tobacco smoke exposes the entire body - every tissue and cell - to powerful mutagens and carcinogens, thus hastening the malignant cellular evolutionary process and accelerating the development of the broad spectrum of neoplastic and degenerative diseases constituting tobaccosis (Table III.8.4).
The differences in mortality among smoking and nonsmoking U.S. veterans amply confirm the pioneering findings of Raymond Pearl, published in 1938, showing a great decrease in the longevity of smokers.
In fact, the life-shortening effects of smoking are now so obvious that it seems incredible that they were generally overlooked for four centuries. Among persons who start smoking in adolescence and continue to smoke a pack of cigarettes daily, the average loss of life is roughly 8 years - approximately equal to the cumulative time actually spent smoking.The most surprising finding of prospective and pathological studies - that the majority of tobaccosis deaths are caused by diseases of the cardiovascular system - initially generated incredulity, and indeed the phenomenon is still not well understood or fully believed by many. It nonetheless deserves full credence and is central to understanding the nature and magnitude of tobaccosis.
The fabric of evidence that cigarette smoking is a major cause of atherosclerosis is woven of these evidential threads:
1. The epidemic increase in ischemic heart disease in the United States during the twentieth century followed the rise in cigarette smoking and occurred particularly among those age-sex subgroups most exposed.
2. Individual studies document a close relationship between heavy cigarette smoking and early coronary disease.
3. There is a plausible pathogenic mechanism by which tobacco smoke could damage vascular tissue: The absorption of inhaled tobacco smoke results in the circulation of polonium 210 and other toxins, with injury to endothelial and other cells, causing cellular damage, clonal proliferation, intramural hemorrhage, lipid deposition, fibrosis,
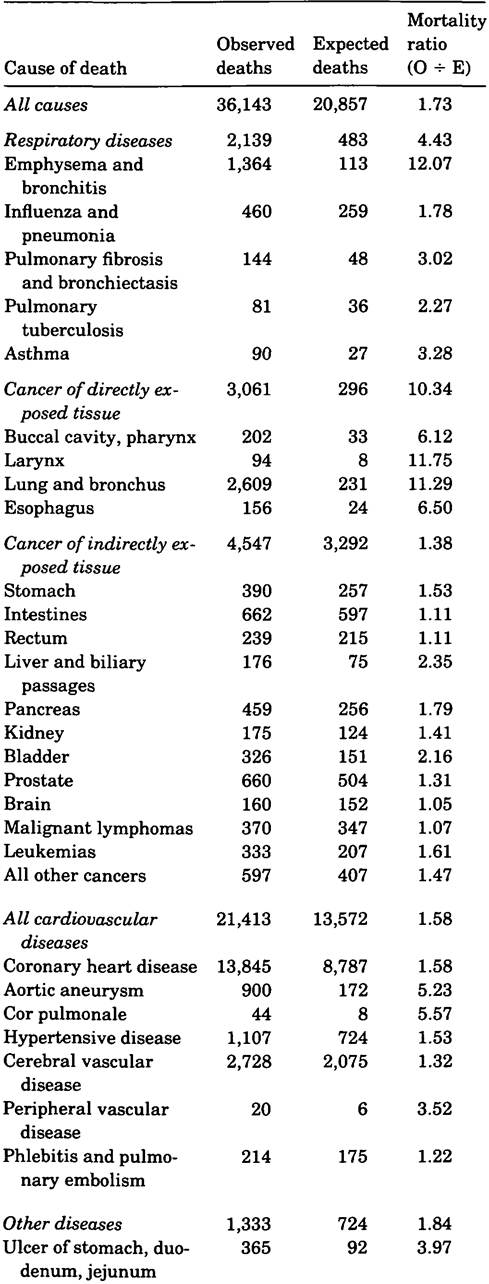
Table III.8.4 Deaths and mortality ratios among smoking U.S. veterans, 1980
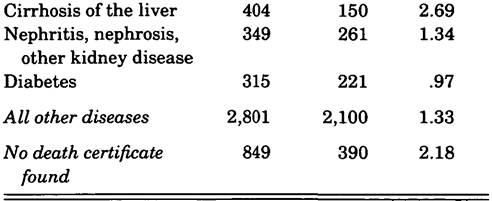
Source: Data from Rogot and Murray (1980).
and calcification. Though often overlooked, ionizing radiation is a powerful cause of atherosclerosis and premature death from cardiovascular disease.
4. Prospective studies of heavy smokers matched with nonsmokers for numerous confounding variables have consistently shown the relative risk of death from atherosclerosis to be much higher for smokers and directly related to the number of cigarettes smoked.
5. Members of certain religious groups that eschew the use of tobacco, such as Seventh-Day Adventists and Latter-Day Saints, have markedly lower morbidity and mortality rates from atherosclerotic disease.
6. Quitting smoking is ordinarily followed by a reduced incidence of coronary heart disease, among specific groups and for the entire population.
7. Experimental studies in animals have demonstrated that tobacco constituents are potent causes of atherosclerotic disease.
The evidence is clear, consistent, and compelling that tobacco smoke is a major cause of atherosclerotic disease and death.
Epidemic Curves
Temporal relationships between twentieth-century epidemic curves for cigarette smoking and death from coronary heart disease, lung cancer, and emphysema/COPD (chronic obstructive pulmonary disease) are presented in Figure ΠI.8.2. The figure shows the massive epidemic of coronary heart disease beginning in the 1920s - a few years after the World War I doubling of cigarette smoking; followed by epidemic lung cancer beginning in the 1930s - 20 “pack years” or 150,000 cigarettes after World War I; followed by epidemic emphysema/COPD beginning in the 1940s - the third decade after World War I. Furthermore, as tar content and per capita cigarette smoking decreased during the last 2.5 years, mortality from coronary heart disease and cerebrovascular disease decreased.
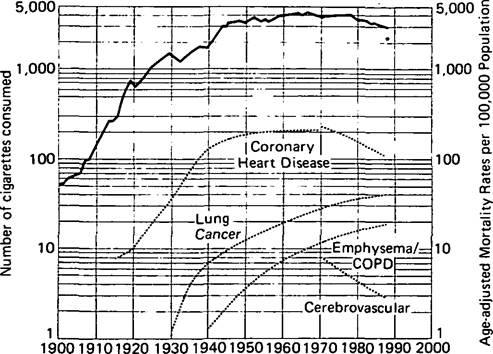
Figure III.8.2. Cigarette consumption and tobaccosis mortality in the United States, 1900-87. The asterisk indicates that the population exposure to tobacco tars is decreasing faster than the cigarette curve. (From Economic Research Service, U.S.
Department of Agriculture; Vital Statistics of the United States; WCHSA Archives [personal communication]; Ravenholt 1962; Walker and Brin 1988; U.S. Department of Health and Human Services.)Magnitude of the Hazard
Although some astute observers attributed lung cancer to smoking during the 1920s, 1930s, and 1940s, there was little general awareness of this relationship until the publication of case-control studies in 1950 showing that almost all (more than 90 percent) of lung cancer patients were smokers. The association of smoking with cancer of the lung was so obvious, consistent, and understandable that many scientists were readily convinced that smoking was the main cause of that disease. But when a number of prominent statisticians (who were themselves smokers) criticized these studies because of possible biases inherent in retrospective studies, massive prospective studies of morbidity and mortality differentials among smokers and nonsmokers were launched about the same time by the British Medical Association, the American Cancer Society, and the American Veterans Administration. (Among the many publications resulting from these studies were those by Doll and Hill [1952], Hammond and Horn [1958], Dorn [1959], and Rogot and Murray [1980].) The studies showed that smokers not only died from cancers of directly exposed tissues of the mouth, larynx, and lungs, but also died at a greatly accelerated rate from a bodywide spectrum of diseases, especially cardiovascular diseases (Table III.8.4) - thus confirming the finding of Raymond Pearl in 1938 that smoking exerted a profound life-shortening effect.
Furthermore, a matched-pair analysis of American Cancer Society prospective data by E. C. Hammond (1964) enabled this author to construct a Lung Cancer Index to total tobaccosis mortality and the estimate of α quarter million U.S. tobaccosis deaths in 1962 - equal to the sum of all deaths from accidents, infection, suicide, homicide, and alcohol.
Truly, for those who smoke a pack or more of cigarettes daily, tobacco is an environmental hazard equal to all other hazards to life combined. In 1967 this estimate was updated to 300,000 deaths for 1966.During two ensuing decades, U.S. lung cancer deaths alone more than doubled from 48,483 in 1965 to 137,000 in 1987. In 1984, with the help of the Multi-Agency Working Group at the National Institute on Drug Abuse, seeking to achieve an updated, realistic estimate of U.S. tobaccosis mortality during the 1980s, this author applied proportionate analytic methods to 1980 U.S. mortality data; 485,000 tobaccosis deaths from cigarette smoking were estimated that year (Table III.8.5), as were
Table III.8.5 Estimated number of deaths caused by cigarette smoking in the United States, 1980
Anatomic site or nature of disease or injury No. of (ICD number) deaths
Malignant neoplasms (140—209, 230—9) 147,000
Diseases of the circulatory system (390-459) 240,000
Ischemic heart disease (410-14) 170,000
Other vascular diseases 70,000
Diseases of the respiratory system other than 61,000 cancer (460-519)
Emphysema (492) 13,000
Chronic bronchitis and other respiratory 48,000
diseases
Diseases of the digestive system (520—79) 14,000
Diseases of the esophagus, stomach, and duode- 2,000 num (530—7)
Cirrhosis and other diseases of digestive system 12,000
Certain conditions originating in perinatal pe- 4,000
riod (760—79) (caused by maternal smoking, low birth weight, and other congenital disabilities)
External causes of injury (E800-E999) 4,000
Injuries caused by fire and flames (E890—E899) 2,500
Other accidental injuries 1,500
Miscellaneous and ill-defined diseases 15,000
Total 485,000
Source: Ravenholt (1984).
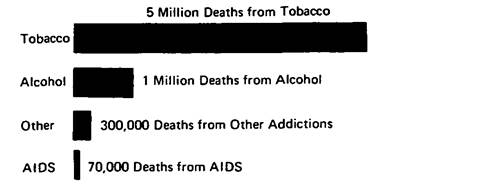
Figure IΠ.8.3. The price of pleasure: deaths from addictive substances and AIDS in the United States, 1980s. (From Ravenholt 1984 and Centers for Disease Control.) more than 500,000 tobaccosis deaths from all forms of tobacco use.
This estimate was accepted and used by the American Council on Science and Health and the World Health Organization, but not by the U.S. Office of Smoking and Health (OSH), which preferred a more “conservative” estimate of 320,000 tobacco deaths in 1987, raised to 390,000 in 1988.
Suffice it to say that the annual tobaccosis death toll - whether the OSH “conservative” estimate of 390,000 or the more complete estimate of 500,000 tobaccosis deaths - is far greater than mortality from any other preventable cause of death in our time and more than 25 times greater than current mortality from the acquired immune deficiency syndrome (AIDS), which emerged during the 1980s as a newly recognized and formidable disease entity (Figure III.8.3).