134 Syphilis
Syphilis or, more properly, venereal syphilis is a chronic communicable disease, which, until the acquired immunodeficiency syndrome emerged in the early 1980s, was the most serious and dreaded of the so-called sexually transmitted diseases (STD) - formerly, venereal diseases (VD).
Caused by Treponema pallidum subspecies pallidum, a spirochetal bacterium, the only known natural host of which is the human being, venereal syphilis is thus one of the human treponematoses - along with pinta, yaws, and endemic syphilis. Although predominantly transferred by sexual contact, T. pallidum is also capable of being transmitted from an infected mother to her fetus across the placenta at any stage of pregnancy (congential syphilis).Syphilis develops naturally through three clinical stages (primary, secondary, and tertiary or late), each separated by a Subclinical period. Of the sub- clinical periods, the one between the secondary and tertiary stages (latent syphilis) is the most pronounced. Clinical manifestations of syphilis are extremely protean, and capable, at the tertiary stage, of affecting any system of the human body.
Syphilis took its name from Girolamo Fracastoro’s well-known poem, Syphilis, siυe morbus gallicus (1530), in which the Italian humanist-physician invented this phrase to name the disease then known all over Europe as morbus gallicus. However, the term syphilis did not become widely used until the late eighteenth century, and that usage was vague and applied to many other symptoms besides those of venereal syphilis until the development of the germ theory in the late nineteenth and early twentieth centuries.
Distribution and Incidence
Unlike human nonvenereal treponematoses (pinta, yaws, and endemic syphilis), venereal syphilis has managed to establish a worldwide distribution, although its incidence patterns are somewhat different in developed and developing countries.
The incidence of syphilis, for example, has continuously declined in the Western world since the 1860s, although major wars have momentarily interrupted this trend. After the Second World War, late and congenital syphilis almost disappeared, mainly as a result of public health measures and penicillin. Since the 1950s, however, both primary and secondary syphilis have steadily increased (nearly 29,000 cases in the United States in 1984) with its peak incidence in the 15- to 34-year age group. A strikingly high male/female ratio (2.6:1 in the United States in 1983) is due to a considerable incidence of syphilis in male homosexuals. In 1980, 58 percent of all syphilitic men in England were homosexuals as were 50 percent in the United States (Csonka 1987; Holmes and Lukehart 1987).
In developing countries, syphilis continues to be a widespread disease, although interpretative problems of serologic tests for syphilis make it difficult to estimate the numbers of infected people in those regions. Syphilis is increasing in areas where yaws was previously endemic, such as tropical and equatorial America and Africa, and Southeast Asia. Infected prostitutes seem to play an important role in the spread of syphilis in these areas, most noticeably in the Far East. The risk of congenital syphilis continues to be considerable in many developing countries, resulting in fetal wastage, neonatal mortality, and infant morbidity (WHO 1986; Csonka 1987).
Etiology and Epidemiology
Although syphilis is transferred predominantly by sexual contact, it may also be transmitted in nonsex- ual ways, such as by close contact with either an open lesion of early syphilis or infected fomites, by
Table VIII. 134.1. Etiology, epidemiology, and clinical manifestations of the human treponematoses
| Venereal syphilis | Endemic syphilis | Yaws | Pinta | |
| Organism | T. pallidum | T. pallidum endemicum | T. pertenue | T. carateum |
| Occurrence | Sporadic, urban | Endemic, rural | Endemic, rural | Endemic, rural |
| Geographic distribution | Worldwide | Southwest Asia, subSaharan regions of Africa, Bosnia | Africa, Southeast Asia, Western Pacific, South America, Caribbean | Central and South America, Mexico |
| Climate in which the disease mostly occurs | All types | Arid, warm | Humid, warm | Semiarid, warm |
| Age group with peak incidence (years) | 18-30 | 2-10 | 2-10 | 15-30 |
| Transmissibility | High | High | High | Low |
| Reservoir of infection | Adults | Children 2—15 years old; contacts in home, school and village; latent cases capable of becoming active | Children 2-15 years old; contacts in home, school and village; latent cases capable of becoming active | Cases with longstanding skin lesions |
| Mode of transmission | Sexual, transplacental0 | Household contacts: mouth-to-mouth or via drinking, eating utensils | Skin-to-skin; ? insect vector | Skin-to-skin; ? insect vector |
| Adult | Early childhood | Early childhood | Adolescent | |
| Primary lesion | Cutaneous ulcer (chancre) | Rarely seen | Framboise (raspberry), or “mother yaw” | Nonulcerating papule with satellites |
| Secondary lesion | Mucocutaneous; occasional periostitis | Florid mucocutaneous lesions (mucous patch, split papule, condyloma latum); osteoperiostitis | Cutaneous papulosquamous lesions; osteoperiostitis | Pintides |
| Tertiary lesion | Gumma, cardiovascular, and CNS lues | Destructive cutaneous Osteoarticular gummas | Destructive cutaneous Osteoarticular gummas | Dyschromic, achromic macules |
“Because the nonvenereal treponematoses are usually acquired in childhood, and because treponemal bacteremia ceases with time, only in adult-onset venereal syphilis is there any likelihood of a mother giving birth to an infected child.
Sources: Adapted from Perine et al. (1984, 2); Perine (1987, 650).infection of an unborn infant in utero, and by transfusions of infected blood.
As noted above, T. pallidum, the causal agent of syphilis, is a member of the order Spirochetales. This order of bacteria includes three genera pathogenic for humans and several other animals: (1) Borrelia, responsible for Vincent’s angina (Borrelia recurrentis), relapsing fever (Borrelia υincentii), and Lyme disease (Borrelia burgdorferi)-, (2) Leptospira, which causes human leptospirosis; and (3) Treponema, responsible for a group of diseases known as treponematoses (Holmes and Lukehart 1987).
The Treponema genus includes several pathogenic species and subspecies responsible for four different human diseases: (1) pinta, a Central and South American disease, which affects the skin, caused by Treponema carateum; (2) yaws, a disease of skin and bones occurring in rural populations of the humid tropics, caused by Treponema pallidum subspecies pertenue; (3) endemic syphilis, similar to yaws, but found only in warm, arid climates, and caused by T. pallidum subspecies endemicum; and (4) venereal syphilis, which has no climatic restrictions and may affect any tissue of the body including internal organs, and is caused by T. pallidum subspecies pallidum. These and other major features concerning the human treponematoses are indicated in Table VΠI.134.1. Surprisingly, in spite of the differentiated (both clinically and epidemiologically) disease entities they produce, these four treponemes cannot be morphologically distinguished from one another. Moreover, they elicit the same immunologic reactions, and are all susceptible to penicillin (Hackett 1963; Perine et al. 1984; Csonka 1987).
Almost from the time of Columbus’s arrival in America, but particularly from the European Enlightenment, the uncertain geographic and historical origins of syphilis have been the object of scholarly controversy (Guerra 1987).
Since the 1950s, however, the rise of molecular biology has pushed anthropologists and historical epidemiologists to frame this problem progressively in terms of the evolutionary origins of all the human treponema- toses. At present, two major theories - the Unitarian and the nonunitarian - contend with each other in providing an explanation for the surprising similarities of the human treponematoses.For E. H. Hudson, the most outstanding defender of Unitarian theory, there is only one treponema- tosis, although it assumes different clinical patterns under different epidemiological conditions. Thus, the changing physical and sociocultural environment of human beings has caused treponematosis to change into one or another of those four different clinical syndromes already mentioned: pinta, yaws, endemic syphilis, and syphilis. From the Unitarian viewpoint, then, it does not make sense to talk about transmission of syphilis from the New World to the Old, or vice versa (Hudson 1965).
By contrast, C. J. Hackett, the main upholder of nonunitarian theory, maintains that the clinical variety of human treponematoses is probably due to mutational changes in the treponemal strains themselves. His thesis is that successive mutations have been responsible for the different human treponematoses starting from a lost ancestral animal treponematosis. The earliest of the treponematoses seems to have been pinta, which might have extended from Africa and Asia into America about 15,000 B.C.; that is, during the last part of the last glaciation and before the subsequent melting of the polar icecaps that formed the Bering Strait.
By about 10,000 B.C., a warm humid environment caused either the pinta treponemes themselves (hypothesis A) or the lost ancestral animal treponemes (hypothesis B) to mutate in Afro-Asia, bringing forth yaws, a disease that extended through Africa, Southeast Asia, and eventually Australia and the Pacific islands, but that did not reach the Americas.
Around 7000 B.C., in the warm arid climates that developed after the last glaciation, another mutation occurred, this time from yaws to endemic syphilis. The latter appeared in northern and Saharan Africa, southwestern and central Asia, and central Australia, whereas yaws itself remained unchanged in the warm and more humid climates.
Finally, about 3000 B.C., the development of large
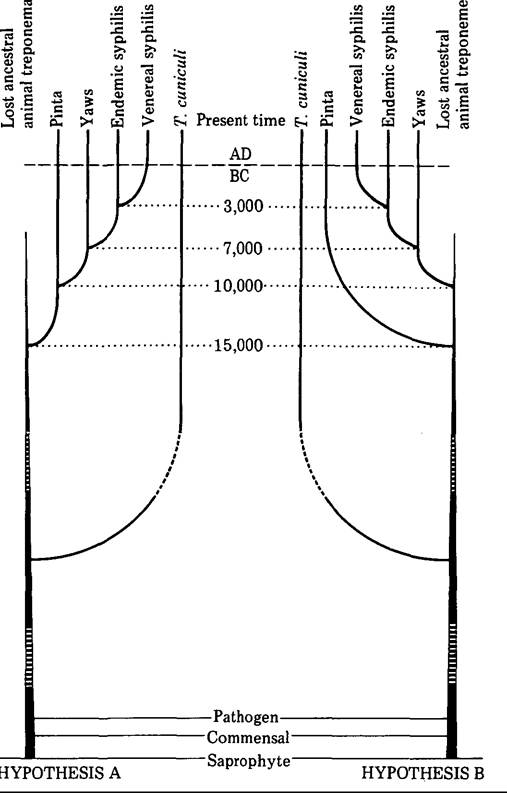
Figure VΠI.134.1. Two hypotheses as to the possible evolution of the organisms responsible for human treponematoses (according to C. J. Hackett 1963, 25). [From C. J. Hackett. 1963. On the origin of the human treponematoses (pinta, yaws, endemic syphilis, and venereal syphilis). Bulletin of the World Health Organization 29: 7-41.]
urban areas and the increasing use of clothing in the eastern Mediterranean and southwestern Asia became selective agents for still another mutation as syphilis changed from a nonvenereal disease of rural children (endemic syphilis) to a venereal disease of urban adults (venereal syphilis). According to Hackett, at any rate, by the first century B.C., as Figure VIII. 134.1 indicates, syphilis had spread throughout the Mediterranean. He suggests, however, that this early venereal syphilis was a “mild” form of the disease, which may explain why there is no evidence of the illness in Europe before the end of the fifteenth century, when a new successful treponeme mutation - probably favored by environmental and social conditions in congested European cities at that time - gave rise to a far more serious disease. Initially extremely virulent, this form of syphilis is supposed to have become progressively less destructive from around the 1530s onward (Hackett 1963). As will be discussed below, however, still other scholars trace the sudden epidemic of venereal syphilis to the post-Columbian importation of an American parasite to Europe, and thence to Asia and Africa.
Immunology
There is no natural immunity to infection by pathogenic treponemes. However, “only about 50 percent of the named contacts of primary and secondary syphilis become infected,” and 25 percent after a single exposure. The chance of infection is influenced - in undefined proportions - by sexual and hygienic practices, inoculum size, environmental and body temperature, and other factors.
Acquired immunity is related to inoculum size and duration of infection prior to treatment. Intradermal inoculation of T. pallidum usually causes primary lesions and serologic response in those who have previously been treated for early syphilis. By contrast, it produces no symptoms or responses in those with untreated latent syphilis, or in those previously treated for late latent (more than 1 year’s duration) syphilis (Holmes and Lukehart 1987).
Clinical Manifestations and Pathology
When William Osler asserted that “who knows syphilis, knows medicine,” he was doing no more than stressing the extreme clinical variety of this disease, which is capable of affecting any system of the human body. As noted previously, the natural course of venereal syphilis includes three consecutive clinical stages, each stage separated by a latent period with no visible signs of infection (Perine et al. 1984; Csonka 1987; Holmes and Lukehart 1987).
Primary Syphilis
T. pallidum penetrates intact mucous membranes and abraded skin. After an incubation period ranging from 2 to 6 weeks (average 3 weeks), the primary lesion — the chancre - appears at the site of entry, it is a single, small, and painless ulcer with undurated edges, usually appearing in the genitalia (penis, vulva, labia, cervix) and, less frequently, in other regions such as the anus, mouth, buttocks, and fingers. Chancres of the penis and vulva are usually accompanied by moderate bilateral enlargement of inguinal lymph nodes. The chancre heals spontaneously over a period of 2 to 6 weeks.
Secondary Syphilis
In most patients, after a brief latent period (6 to 8 weeks), there is a secondary clinical stage characterized by the appearance of disseminated lesions on the skin and in the internal organs. In women, these lesions are often the first overt clinical sign of syphilis. Secondary lesions consist of a symmetrical, evolutive, and painless rash, very variable in appearance and localization, and usually accompanied by fever, malaise, aches in the bones (often worse at night), and generalized enlargement of lymph nodes. After a few weeks - generally 2 to 6 - secondary lesions and symptoms spontaneously disappear. In 25 percent of untreated patients, however, there is a recurrence of secondary lesions during the first 2 years of infection.
Tertiary or Late Syphilis
The tertiary stage develops only in about one-third of untreated cases, and only after another latent period lasting from 1 to 20 years, or even longer. This stage is characterized by progressively destructive lesions of the skin and mucous membranes, bones, and internal organs. The most typical lesion is the gumma, a small rubbery tumor that is a benign manifestation of tertiary syphilis, which can develop in any part of the body.
Particularly serious forms of late syphilis involve the cardiovascular and central nervous systems. Cardiovascular syphilis may cause aneurism of the thoracic aorta, and dilatation of the aortic valve. Neurosyphilis includes a loss of positional sense and sensation (tabes dorsalis, locomotor ataxia) or a form of insanity (general paresis [GPI], dementia paralytica).
As a result of the introduction of antibiotic therapy, tertiary syphilis has almost disappeared. Thus the most reliable information available on it today has been provided by two major studies on the course of untreated syphilis, the Oslo Study (1891-1951) and the Tuskegee Study (1932-72). The former surveyed retrospectively a group of nearly 2,000 patients with primary and secondary syphilis diagnosed clinically before immunologic tests came into use. The latter studied prospectively 431 black men with seropositive latent syphilis of 3 or more years’ duration, who were deliberately kept untreated. Because of the ethical issues raised by this racist experiment, the Tuskegee Study has been crucial in formulating the present guidelines concerning medical experimentation on humans (Jones 1981; Holmes and Lukehart 1987).
Congenital Syphilis
The risk of congenital syphilis to the fetus is high during the first 2 years after the mother has acquired the infection. An infected fetus may die during pregnancy, be stillborn, or be bom prematurely. Secondary-type lesions are present at birth or appear within the first 6 months of life (Perine et al. 1984; Csonka 1987; Holmes and Lukehart 1987).
History and Geography
Medical historiography has in the past usually identified the disease known today as venereal syphilis with the morbus gallicus that was mentioned for the first time in European medical and lay writings of the late fifteenth century. Indeed, nineteenth- and twentieth-century medical historians, in looking at past medical and lay descriptions of morbus gallicus, have systematically practiced a retrospective diagnosis of syphilis.
According to them, the history of syphilis began with the eruption of morbus gallicus in Europe in the 1490s, and can be traced throughout the centuries until today, although neither its geographic origins nor the precise date of its appearance has been established. Since the European Enlightenment, both of these questions have been the object of a continuous - and often tart - controversy between the defenders of an American origin of syphilis and those who have claimed that syphilis did exist in the Old World long before Columbus arrived in the New World. The most varied documental proofs (medical and lay writings, iconography) and - increasingly since the late nineteenth century - material proofs (paleopathological remains) have been wielded in this debate. It is an unfinished debate, however, for in claiming that present-day venereal syphilis was already known and had been described under several names before or after the Europeans’ arrival in America, historians have produced the kind of contradictory conclusions that serve only to keep it alive (Guerra 1978; Wood 1978).
A second way of approaching the history of syphilis has already been referred to in the section on the etiology and epidemiology of syphilis. This approach lies in studying the disease and the germ responsible for it in the broad biological and epidemiological context of the development of human treponema- toses, and integrates results provided by both paleopathological and historicoepidemiological studies. A result of this approach has been some attractive and promising hypotheses on the history of syphilis, but at the moment, no definitive conclusions have
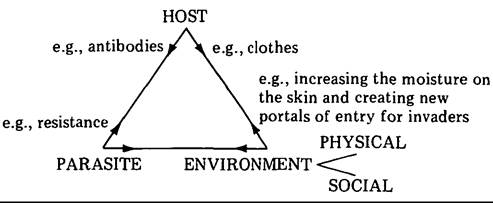
Figure VIIL 134.2. Infectious diseases considered as a dynamic triangular interaction among host, parasite, and environment (according to E. H. Hudson, 1958, 8-9.) (Adapted from E. H. Hudson. 1958. Non-Venereal syphilis. Edinburgh-London.)
been reached (Hackett 1963; Hudson 1965; Wood 1978).
Given these circumstances, a third approach seems appropriate, which actually deals with the history of the concept of syphilis, rather than with the history of the disease itself. This third way renounces retrospective diagnosis of syphilis and insists on the need to contemplate the disease entity called syphilis within the strict historicocultural context in which it occurs, and from which it receives its true significance. Put plainly, every disease entity is an intellectual construction that is peculiar to some form of medicine; and every form of medicine is nothing but a historical variable in any human community. Thus the disease entity known today as venereal syphilis can be conceived of, at this point, as a paradigmatic example as was demonstrated by a Polish microbiologist, Ludwik Fleck, in the mid-1930s in a monograph in which there has been renewed interest since the late 1970s (Fleck 1979).
Furthermore, in looking at what we call infectious diseases, we must distinguish between what may be termed disease entities and the diseases themselves. As disease entities, infectious illnesses assumed their present shape only in late nineteenth- and early twentieth-century Western medicine as a result of the development of germ theory. But as diseases in themselves they have existed for a long time.
Infectious diseases, moreover, cannot be regarded ontologically as natural beings in the same way as the microbiological agents that cause them can be regarded (Reznek 1987). Rather, as Hudson (1958) has demonstrated, in the case of human treponema- toses, they should be considered the result of a dynamic interaction among host, parasite, and environment, as portrayed in Figure VΠI. 134.2. Moreover, any such interaction that has occurred in the past can neither be reproduced under experimental conditions, nor be easily reconstructed historically.
To be precise, venereal syphilis took shape in Western scientific medicine only as a result of deep changes, both intellectual and social, during the second half of the nineteenth and the first decade of the twentieth century; foremost among these changes was the formulation of germ theory. Yet an exhaustive bibliographical survey on venereal diseases done by J. K. Proksch in 1889-1900 makes clear that the term syphilis, though invented by Fracastoro in the sixteenth century, did not become widely used until the late eighteenth or early nineteenth century. So, it may be anachronistic to refer to as syphjlis either the disease entity that we call “venereal syphilis” before the late nineteenth or early twentieth century, or a disease entity named “syphilis” before the late eighteenth or early nineteenth century.
Let us now consider the origins, emergence, and development of the concept of syphilis. Our departure point will be the disease entity that began to be called morbus gallicus in late fifteenth-century Europe. Although for the above-mentioned reasons we cannot agree with those who have identified morbus gallicus with syphilis, it is obvious that the former may well be considered the earliest identifiable conceptual ancestor of the disease entity that we now call venereal syphilis (Fleck 1979).
1400—1600
Morbus gallicus is the name that soon became dominant in designating a disease generally considered as new in Europe of the 1490s. It was perceived as an incurable and loathsome disease consisting of severe aches in the bones, and of sores usually beginning in the genitals, but eventually covering most or all of the body. Contemporary medical and lay evidence concurred in including it among the numerous calamities (floods, earthquakes, epidemics, famines, wars) that Europeans - especially Italians - suffered at the end of the fifteenth century.
Italian sources show us that the “French Pox” spread in Italy during the period 1494-5, after the clash between the armies of France and Spain over the question of the kingdom of Naples. The notoriety the phrase morbus gallicus soon achieved all over Italy was closely associated with the tragic consequences of the impact of the French invasion on the fragile Italian political equilibrium. Similarly, the prompt acceptance in early sixteenth-century Italy of the theory of an American origin for morbus gallicus may be explained by the fact that Spaniards were regarded as the newest barbari Stranieri to devastate Italy. The great prestige of Renaissance Italy and its cultural hegemony throughout Europe were important factors, among others, in ensuring the rapid popularization of both the term morbus gallicus and the theory of its American origin.
Through the sixteenth century, the phrase “French Pox” achieved in Europe and overseas an overwhelming dominance over any other names for the disease, not only in the medical academic world, but also at popular levels. Only French physicians - those native to or settled in France - seem, understandably, to have rejected this name, and put forth others. For example, in 1552 Thierry de Hery of Paris suggested maladie venerienne or grosse υairolle; in 1553 Auger Ferrier of Toulouse proposed pudendagra or lues hispanica; in 1560 Antoine Chaumette of Paris put forth the denomination morbus υenereus; and in 1563 Leonardo Botallo, also of Paris, used the term lues venerea, as did Jean Fernel in posthumous publication in 1579.
1600-1750
During the seventeenth century this new term, lues venerea (venereal disease), was adopted all over Europe, sharing an ex aequo leadership with that of morbus gallicus. In eighteenth-century Europe the term “lues venerea” eventually superseded that of morbus gallicus, and the use of the latter declined dramatically.
Two points may be raised about the expression lues venerea. First, the adjective “venerea” stresses the direct relationship existing between the French Pox and the pleasures of Venus and, thus, the individual responsibility of those who contract the disease. Applied to the morbus gallicus, this adjective seems to have appeared for the first time in 1527 in a work by French physician Jacques de Bethencourt, entitled Nova poenitentialis Quadragesima, nec non Purgatorium in Morbum Gallicum sive Venereum. Both the title and contents of this book evoke the climate of religious exaltation and of moral rearmament present in Reformation Europe (Temkin 1977). The second point has to do with the name “lues,” which underscores the perception of the disease, at that time, as a contagious and calamitous one from a physical, and even from a moral, viewpoint.
A good example of the dominance exerted by the expression “lues venerea” on eighteenth-century European university medicine is offered to us by an influential work of the French royal physician Jean Astruc, De Morbis Veneris, published in 1736, which was reissued many times and translated into a great
number of European languages before the end of the nineteenth century. The work argues that the lues venerea was caused by a unique and specific virus venereum. It treats the particular morbi venerei as species making up the genus Lues venerea, and it differentiates between lues venerea incipiens and confirmata. The first was composed of different morbi venerei (gonorrhea, hernia venerea, bubones venerei, caries pudendorum, and porri, among others); whereas the second, the lues venerea confirmata, also called morbus venereus universalis, comprised numerous complaints affecting the whole human body. Among these were morbi genitalium, vitia cutis, morbi oris et narium, dolores venerei, morbi ossium, tumores, glandulosi et lymphatici, oculorum morbi, morbi aurium, and Iesiones functionum.
1750-1850
Whether venereal disease was caused by an animated contagion or by a chemical poison, until the mid-eighteenth century almost every intellectual stream in European academic medicine seems to have defended the unity of lues venerea on the basis of a unique and specific virus venereum. However, after 1750 the concept of lues venerea began to be challenged as a result of nosographic and nosological efforts made by Enlightenment pathologists, who (with the support of clinical observations, anatomopathological analyses, and inoculation experiments) began to question whether lues venerea was a single disease entity after all. The result of this challenge was the progressive disappearance of the expression lues venerea from the literature. And although it did not entirely disappear until the nineteenth century, it was increasingly replaced by the plural expression morbi venerei (venereal diseases), which began to be used at the beginning of the eighteenth century. At about the same time, specific denominations given to each one of the “morbi venerei” (chancre, gonorrhea, bubo, and syphilis, among others) started to appear with increasing frequency. From the early nineteenth century, the number of medical works specifically devoted to certain among these diseases - mainly to gonorrhea and syphilis - began to proliferate.
Let us look in more detail at how the concept of lues venerea was destroyed during the period 1750-1850, while keeping in mind that it was during this period that specialized hospitals emerged, including those for the treatment of venereal disease and that dermatovenerology was bom as a medical specialty. Enlightenment controversies over lues venerea came to concentrate mostly on whether the Mennorrhagic discharge - usually called gonorrhea - happening in many venereal patients, constituted a disease entity different from lues venerea, or (as thought before), was just a peculiar clinical form or stage of lues venerea (Flegel 1974). The beginning of this process of disease differentiation, which, roughly speaking, took place in Europe and North America throughout the century 1750—1850, may be found in the influential work by Giovanni Battista Morgagni, De Sedibus et Causis Morborum per Anatomen Indagatis, published in Venice in 1761. He found at autopsy that venereal patients with Hennorrhagic discharge and no evidence of chancre rarely had hidden in the genital passages the expected chancre, which was supposed to provoke the discharge in the first place.
During the following decades, numerous physicians argued the single or dual nature of lues venerea, resorting to anatomoclinical observations and to autoinoculative and heteroinoculative experiments with pus from venereal lesions. This controversy did not end until the 1830s in part, at least, because there was tremendous ambiguity in the use of terms referring to venereal complaints. Although terms like syphilis, maladie(s) syphilitique(s), and so forth spread rapidly in the European medical literature during the first two decades of the nineteenth century, the term syphilis became almost dominant after the 1820s. The word nonetheless continued to appear in some works as an alternative term or one complementary to that of “venereal diseases.”
The controversy, however, over whether venereal disease was a single disease entity or more than one illness was brought to an end in the late 1830s. During this period the French venereologist Philippe Ricord had developed a vast clinical and experimental program at the Paris Hopital du Midi, including both the systematic use of the uterine speculum and numerous (more than 2,500) autoinoculative experiments with pus from venereal patients. In 1838 he presented his results and conclusions in Traite pratique sur les maladies υeneriennes, ou recherches critiques et experimentales sur Vinoculation appli- quee a Vetude de ces maladies. These experiments, asserted Ricord, had permitted him to demonstrate the existence of the so-called virus Syphilitique, so that chancre and Hennorrhagia could be definitely separated. Moreover the expectations had also allowed him to distinguish the primary lesions of verole from those that are not primary, and primary symptoms from secondary symptoms. As a result, Ricord proposed the division of syphilis symptoms into primary, successive, secondary, transitional, and tertiary.
1850—1950
During the second half of the nineteenth and the beginning of the twentieth century, Ricord’s concept of syphilis was gradually reshaped, as other disease entities recognized today as sexually transmitted diseases (gonorrhea, chancroid, lymphogranuloma venereum, genital herpes, venereal warts, and others) were emerging. If most of these new disease entities were first shaped according to anatomoclini- cal criteria, each one of them (syphilis included) eventually got its definitive “identity card” when the relevant germ causing it was isolated.
Gonorrhea and chancroid are two illustrative examples in this respect. Ricord, who definitely separated chancre and blennorrhagia, asserted that the latter might be the result of local irritation, excessive sexual intercourse, or excessive sexual excitement. The present clinical picture of gonorrhea was completed only in 1879, when Albert Neisser discovered the germ responsible for it, which he called gonococcus. On the other hand, chancroid or soft sore (ulcus molle) emerged as a disease entity in 1852, when a pupil of Ricord, Leon Bassereau, demonstrated that the two kinds of luetic chancre - one hard, painless, and unique; the other soft, painful, and frequently multiple - resulted from exposure to a like lesion. In addition, the latter was autoinocula- ble. Almost 40 years later, in 1889, August Ducrey identified the bacillum responsible for it (Kamp- meier 1984).
As for the concept of syphilis, it developed and changed profoundly during the second half of the nineteenth century as the disease became a major research area in Western scientific medicine. Perhaps the person who contributed most to the development of the concept of syphilis during this period was the French venereologist Jean-Alfred Foumier. It was Foumier who propounded the concept of latency in both acquired and congenital syphilis, definitely established the relationship between syphilis and so-called parasyphilitic affections (mainly tabes dorsalis and general paresis of the insane), and began a social campaign against the disease.
But the discovery of the germ responsible for syphilis did not occur until 1905, when Fritz Schaudinn and Erich Hoffmann isolated it in serum from a lesion of secondary syphilis. In 1906 the collective work of August von Wassermann, Albert Neisser, Carl Bmck, and others made possible the invention, in Germany, of the first serologic procedure for the diagnosis of syphilis. This was the complementfixation test, which soon became well known as the Wassermann Reaction (WR). In the following years, T. pallidum was also found in lesions of tertiary syphilis, verifying Fournier’s theory. Karl Reuter, for example, in 1906 found the germ in the wall of a syphilitic aorta, whereas Hideyo Noguchi in 1913 proved its presence in brain tissue from paretics (Quetel 1986).
By way of conclusion it should be emphasized that, as has been the case with many other disease entities, a crisis of a disease entity concept based upon its specific biological cause (Lafn-Entralgo 1982) has also ensnared venereal syphilis. In 1935, whereas most bacteriologists and pathologists still claimed specificity of a causal microorganism to be the definitive nosographic criterion for an infectious disease, Fleck lucidly insisted upon the essential incompleteness of the concept of syphilis (Fleck 1979).
Time has confirmed Fleck’s insight. Put plainly, it should be obvious from the foregoing that Western medicine has had enormous difficulties in establishing scientific criteria that delimit precisely the so- called venereal syphilis from the remaining human treponematoses (Hackett 1963; Hudson 1965; Perine et al. 1984).
Jon Arrizabalaga
Bibliography
Baker, Brenda J., and George J. Armelagos. 1988. The origin and antiquity of syphilis: Paleopathological diagnosis and interpretation. Current Anthropology 29: 703-37.
Bardet, Jean-Pierre, et al. 1988. Peurs et terreurs face a la contagion: Cholera, tuberculose, syphilis: XlX-XXe socles. Paris.
Crosby, Alfred W. 1972. The Columbian exchange: Biological and cultural consequences of 1492. Westport, Conn.
Csonka, G. W. 1987. Syphilis. In Oxford textbook of medicine, 2d edition, ed. D. J. Weatherall et al., Vol. 1: 5.386-5.403. Oxford.
Fleck, Ludwik. 1979. Genesis and development of a scientific fact, trans. Fred Bradley and Thaddeus J. Trenn, ed. Thaddeus J. Trenn and Robert Merton. Chicago- London.
Flegel, Kenneth M. 1974. Changing concepts of the nosology of gonorrhea and syphilis. Bulletin of the History OfMedicine 48: 571—88.
Grmek, Mirko. 1988. Diseases in the Ancient Greek world. Baltimore.
Guerra, Francisco. 1978. The dispute over syphilis: Europe versus America. Clio Medica 13: 39-61.
Hackett, C. J. 1963. On the origin of the human treponematoses (pinta, yaws, endemic syphilis and venereal syphilis). Bulletin of the World Health Organization 29: 7—41.
Holmes, King K., and Sheila A. Lukehart. 1987. Syphilis. In Harrison’s principles of internal medicine, Ilth edition, ed. E. Braunwald et al., 639-49. New York.
Hudson, E. H. 1958. Non-Venereal syphilis. Edinburgh- London.
1965. Treponematosis and man’s social evolution. American Anthropologist 67: 885-901.
Jones, J. H. 1981. Bad blood: The Tuskegee syphilis experiment. New York and London.
Kampmeier, Rudolph H. 1984. Early development of knowledge of sexually transmitted diseases. In Sexually transmitted diseases, ed. K. K. Holmes et al., 1929. New York.
Lain-Entralgo, Pedro. 1982. El diagnostico medico: Historia y teoria. Barcelona.
Perine, Peter L. 1987. Nonvenereal treponematoses: Yaws, pinta, and endemic syphilis. In Harrison’s principles Ofinternal medicine, Ilth edition, ed. E. Braunwald et al., 650-2. New York.
Perine, Peter L., et al. 1984. Handbook of endemic treponematoses. Geneva.
Proksch, J. K. 1889-1900. Die Literatur uber die υen- erischen Krankheiten von den ersten Schriften iiber Syphilis aus dem Ende des filnfzehnten Jahrhun- derts..., 5 vols. Bonn.
Quetel, C. 1986. Le mal de Naples: Histoire de la syphilis. Paris.
Reznek, Lawrie. 1987. The nature of disease. London and New York.
Temkin, Owsei. 1977. On the history of “morality and syphilis.” In The double face of Janus and other essays in the history of medicine, ed. O. Temkin, 472-84. Baltimore.
Wood, Corinne Shear. 1978. Syphilis in anthropological perspective. Social sciences and medicine 12: 47-55.
World Health Organization. Expert Committee on Venereal Diseases and Treponematoses. 1986. Sixth report. Geneva.
More on the topic 134 Syphilis:
- 134 Syphilis
- Contents
- Name Index
- Kiple Kenneth F. (Editor). The Cambridge World History of Human Disease. Cambridge University Press,1993. — 1200 p., 1993
- Index