64 Herpes Simplex
Herpes simplex is caused by Herpes virus hominis, of which there are two distinct serologic types designated as HSV-I and HSV-2. The first mainly causes disease above the waist, such as cold sores; the second most commonly causes disease below the waist, especially genital herpes.
Exceptions to this generalization occur especially among the newborn. The initial active phase is followed by prolonged latency. But the virus can be reactivated by another infection, stress, exposure to sunshine, or any number of other bodily changes.Etiology and Epidemiology
The herpes viruses are visible in infected cells by electron microscopy and may be grown in the chick embryo, in tissue cultures, and in laboratory animals that react differently to types HSV-I and HSV-2.
HSV-I is shed from cells in the lacrimal and salivary glands, and both types are shed from the primary and recurrent lesions of the mucous membranes and skin. Samples of infected adults show that 2 to 4 percent are excreting the virus at a given time.
Infection with the herpes simplex virus results from person-to-person contact. HSV-I infections commonly are transmitted by oral secretions through kissing or the sharing of eating utensils, and thus herpetic infection can easily be spread within a family. Normally HSV-I infections are painful and bothersome but have no serious consequences. An exception can be when the virus invades the cornea of the eye. Conjunctival or corneal herpes may produce scars that impair vision. It may occur among wrestlers from skin-to-skin contact. Another form of HSV-I infection, called herpetic paronychia, may occur in dentists and in hospital personnel.
HSV-2 infections are generally the result of sexual transmission at a time the virus is being shed. Lesions appear on the penis, vulva, buttocks, and adjacent areas, and the mucosa of the vagina and cervix.
The prevalence of HSV-2 infection during pregnancy and its incidence in neonates are related to the socioeconomic level, age, and sexual activity of a population. In one urban population study, 35.7 percent of women attending an obstetrical clinic had serologic evidence of past HSV-2 infections. Moreover, of these women in a study of a lower socioeconomic sample, the antepartum infection rate was 1.02 percent. The infant was safe from infection if the mother’s infection had cleared 3 to 4 weeks before delivery. On the other hand, the experience of283 women with genital herpes suggests that those women who suffer from genital herpes during pregnancy are three times more likely to abort than other women during the first 20 weeks of pregnancy. In this same study, the risk of neonatal infection was 10 percent if infection occurred after 32 weeks of pregnancy, and increased to 40 percent if infection was present at confinement. Neonatal infection from infected mothers is almost certainly of the HSV-2 type, acquired by passage through an infected birth canal. In addition HSV-2 may be transmitted from infant to infant in the hospital nursery by its personnel.
The epidemiology of recurrent herpes is complicated by unknown factors that cause reactivation of the virus. Because the epidemiology of recurrence depends on recollection, the most acceptable studies of reccurent herpes Iabialis come from students in health care professions. These show inexplicable differences in recurrence: 45 percent in Wales and the United Kingdom, 40 percent in North America, 30 percent in Europe and Africa, 17 percent in Asia, and 16 percent in South America.
The possible relationship of HSV-2 to carcinoma of the cervix has been explored in recent years in light of its ability to transform cells in vitro, the incidence of antibodies to HSV-2 in cancer patients, and the demonstration of viral RNA in cancer cells from the cervix. No conclusive studies have been published to date.
Distribution and Incidence
Infection by herpes virus is reported worldwide, as determined by antibody studies, and is related to the socioeconomic state.
The prevalence of positive antibody tests to HSV-I approaches universality (100 percent) in the lower strata, falling to 30 to 50 percent among those of higher socioeconomic levels. Obviously, transmission is more likely among those living in a crowded and unhygienic environment. The prevalence of positive antibody response begins in early childhood and rises to its peak in adult life. Transplacental antibodies are present in infants up to 6 months of age. Then a sharp rise in antibodies occurs for those aged 1 to 4 years, mainly to HSV-1. This is followed by a slight rise from 5 to 14 years, and after 14 there is a marked rise in antibodies through late adulthood, which is in part due to HSV- 2 infection (see Figure VIII.64.1).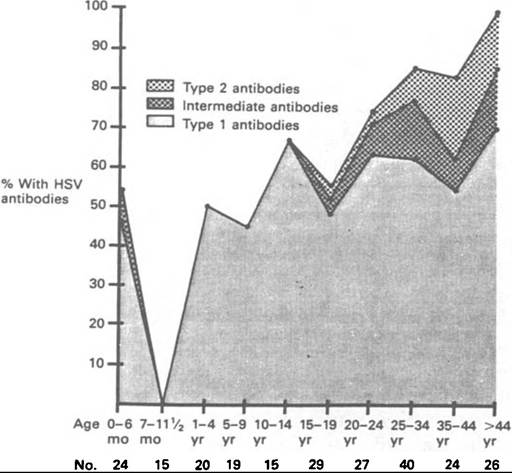
Figure VIIL64.1. Percentage distribution of antibodies to HSV-1, HSV-2, and intermediate form (types 1 and 2) in 239 patients of various age groups. (From A. J. Nahmius and D. E. Campbell. 1983. Infections caused by herpes simplex viruses. In Infectious Diseases, 3d edition, ed. Paul D. Hoeprich, 859, by permission of Harper & Row, publishers.)
Because HSV-2 infection is a sexually transmitted disease, it has been studied more intensively in recent years than the more common HSV-I infection.
On the other hand, most observers agree that herpes genitalis has been on the increase in recent years, and in 1983 the National Institutes of Health estimated that there were 20 million cases in the United States, with 300,000 to 500,000 new cases developing annually. Undoubtedly, contributing factors include increased sexual activity as well as a preference for the use of oral contraceptives over the condom, although a wider use of diagnostic tests may account for some of the apparent increased prevalence. Certainly, publicity concerning herpes genitalis has alerted the medical profession to the disease and has made the public aware that “chafing of a menstrual pad” and lesions on the male genitals may entail more than temporary annoyance.
In any event, beginning with its 1983 Annual Summary, Morbidity and MortalityReports, the U.S. Public Health Service has included herpes genitalis. The report for 1984, based on physician consultations, office visits, and the first office visits for the disease, “reflects a 16 fold increase from 28,000 to 423,000 in the number of consultations for genital herpes in the period 1966-1983” (see Figure VIII.64.2).
Immunology
Antibodies to the herpes viruses last throughout the patient’s lifetime. An antigen common to both HSV- 1 and HSV-2 produces crossreacting antibodies to both strains that can be differentiated immunologically by immunofluorescence and microneutralization tests. Antibody to one type, however, precludes neither an infection with the other nor the development of specific antibodies to the second infection. Yet previous infection with HSV-I does mitigate the clinical manifestations of the first episode of genital herpes caused by HSV-2. The antibodies that respond to an initial herpes simplex virus infection are complement-fixing, neutralizing, cytotoxic, precipitating, and nonprecipitating antibodies, and appear early in the infection. Lawrence Corey (1984) has stated that although complement-fixing and neutralizing “antibodies usually are maintained and in high titer, and inactivate extracellular virus, continued replication of virus by cell to cell transfer ensues. These data help explain frequent reactivation of the disease in the presence of high levels of antibody titer.” The relation of humoral antibodies to reactivation of disease is unclear. Whereas the humoral immune response remains at high levels, the in vitro cellular immune response to HSV antigens appears to fluctuate.
Figure VIII.64.2. Number of consultations, all five office visits, and first of five visits for genital herpes, United States, 1966—83. All consultations (solid line) include any type of patientphysician interaction, such as telephone calls, house calls, and office visits.
[From U.S. Public Health Service. Centers for Disease Control. 1984. Morbidity and Mortality Weekly Reports, Annual Summary (March) 33: 90.]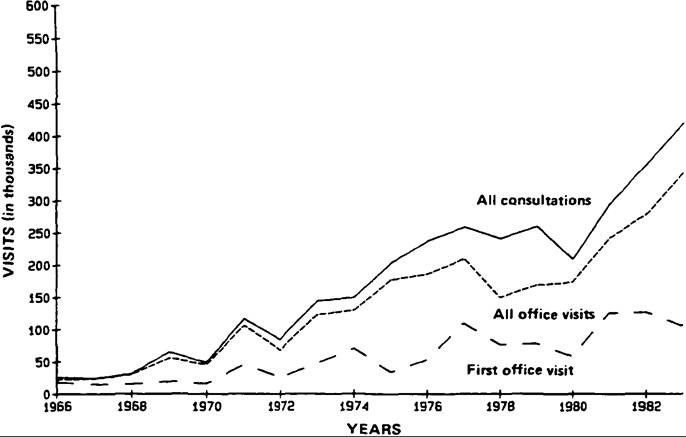
Pathology and Clinical Manifestations
The virus multiplies in the epithelium at the portal of entry. The epithelial cells increase in size and contain an enlarged nucleus with intranuclear inclusions. The developing blisterlike vesicle is intradermal and is surrounded by inflammatory cells, edema, and congestion. Viremia may develop in malnourished infants as an accompaniment to measles, and in patients with extensive burns or in those on immunodepressant drugs. Systematic disease accompanies viremia.
The initial lesion at the site of inoculation or at the site of recurrence, whether in the skin or mucous membrane, is a small reddened area that develops into a small, thin-walled, blisterlike vesicle filled with clear fluid. Equally as common is the appearance of a group of small vesicles on the erythematous base.
Gingivostomatitis is the usual type of primary or initial HSV-I lesion in infants and young children and is seen occasionally in adults. There may be several days of prodromal symptoms such as malaise, fever, and usually cervical Iymphadenopathy. Commonly, by the time a physician is consulted, the gums are inflamed and ulcerated. Pain is distressing and may interfere with eating; the course is normally a week to 10 days.
Labial herpes only occasionally represents the initial HSV-I lesion, but the “cold sore” or “fever blister” of the lip is the most common lesion of recurrent disease. Here a cluster of vesicles appears after a couple of days Ofhyperesthesia and erythema, to last from several to 10 days. Most commonly these appear at the vermilion line of the skin of the lower lip or on the skin of the upper lip, at times extending to or into the nostril. The term “fever blister” stems from the frequency with which herpetic recurrence accompanies febrile illnesses.
Before the age of antibiotics, it was more likely to accompany pneumococcal pneumonia than other types of pneumonia or febrile disease.Conjunctivitis with or without keratitis may be the primary lesion of herpes virus infection. Then the preaιuicular lymph node commonly is enlarged. Keratitis is characterized by dendritic ulceration.
Cutaneous herpes (HSV-I) may involve the skin of the body, anywhere above the waist and including the feet. (HSV-2 has been isolated from fingers from autoinoculation or genital-to-finger contact in sexual play.) It may be accompanied by edema, fever, lymphangitis, and Iymphadenopathy.
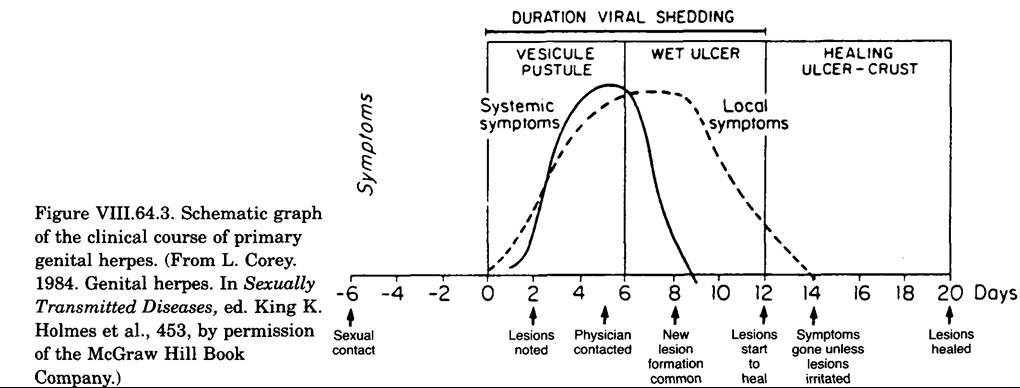
Herpes genitalis also has the incubation period of several days following exposure to infection. It may be Subclinical, especially in women having lesions only in the vagina or the cervix rather than on the vulva. Herpetic infection is more obvious in men with localized pain, erythema, and the development of one or a group of vesicles on the glans, prepuce, or elsewhere on the penis. The inguinal lymph nodes may be swollen and tender. Urethral involvement in both sexes is manifested by dysuria (painful or difficult urination), and a discharge may be noted in male patients. Pelvic pain accompanying the dysuria is common in women. (The virus can be isolated from the urethra of both sexes. Primary infection with HSV-2 virus often is accompanied by systemic symptoms during the first several days (see Figure VIII.64.3). Complications of primary infection reveal a generalized infection, especially as aseptic meningitis and other indications of viral invasion of the central nervous system.
In a study of 148 newborns with herpes, A. J. Nahmias and colleagues (1970) reported an incubation period of up to 21 days; almost all were infected with HSV-2 and had evidence of dissemination. The overall fatality rate was 71 percent, and 95 percent among those with disseminated infection. Of those recovering, 15 percent had sequelae, especially defects in the central nervous system.
Some studies show recurrences within the first year in 80 percent of infections with HSV-2. Recurrent lesions commonly present with milder symptoms initially, are generally of shorter duration, and are rarely accompanied by overt systemic symptoms. These lesions commonly appear on the genitalia, but may appear on the buttocks and elsewhere adjacent to the genital area. Latent infection presumably is established in the sacral-nerve-root ganglia. From a study of 375 patients, Stanley Bierman (1983) found that recurrences ceased in half of them after some 7 years following the onset of disease. In others, however, the recurrences may span many years.
It is unclear what triggers recurrent genital herpes. Emotional stress, fever, heat, trauma, coitus, and the menses have all been suggested. But they lack the certainty that a febrile illness seems to play as a provoking factor in HSV-I recurrences.
History and Geography
The word herpes is derived from the Greek verb “to creep,” and the identification of disease in ancient writings depends upon one’s interpretation of the description of physical signs. Thus, one may decide either that a described lesion was of the herpetic type or accept the translation of the term “herpes” itself. No doubt aphthae and herpetic lesions were not differentiated.
The oldest record of disease of the genitalia appears in the Ebers Papyrus (c. 1550 B.C.). The translator commented on the inflammation of the vulva and thighs of a woman in nonspecific terms, but in the same papyrus describes treatment for “herpes of the face.” Hippocrates spoke of “herpetic sores” and, again in his Epidemics, that “many have aphthae and ulcerations of the mouth, frequent Auxations of the genital organs and ulcers.” Herodotus described herpetic eruptions “which appear about the mouth at the crisis of simple fevers.” H. Haeser (1875), in reviewing the medical writings of the Byzantine Empire, quotes from three physicians (the fourth to seventh centuries) concerning “superficial aphthae” and “vesicular eruptions” of the vulva. J. Preuss (1911), a Biblical scholar, in referring to the Talmud’s permission to delay the rite of circumcision, said, “Mila betzaraath is probably harmless herpes of the foreskin.”
The first definitive description of herpes appears in Jean Astruc’s 1736 publication of De Morbis Venereis, translated into English and published in London in 1754. His description of vesicles in both male and female patients unmistakably indicates those ofherpes genitalis. Toward the end of the eighteenth century, the English physician Robert Willan developed a classification, published in 1808, of the bewildering varieties of skin diseases, among which was a category of vesiculae.
In his Synopsis of Cutaneous Diseases (1818), Thomas Bateman described herpes Iabialis, which “occasionally appears as an idiopathic affection... frequently in the course of disease of the viscera of which it is symptomatic.” His accurate description of herpes praeputialis emphasized the hazard of interpreting a cluster of vesicles as a syphilitic chancre. He described the prodromes, development of the erythema and vesicles, and their course to healing, ending with, “I have not been able to ascertain the causes of this eruption on the prepuce.... Whencesoever it may originate, it is liable to recur in the same individual at intervals of six or eight weeks.”
Jean Louis Alibert (1832) not only described herpes praeputialis but stated that the lesion may occur at the introitus of the vagina. F. L. Legendre (1853) described three instances of herpes of the vulva, with the observation that herpes may recur 2 or 3 days before menstruation.
The most descriptive paper on herpes progenitalis was presented by Boston physician F. B. Greenough (1881), at the meeting of the American Dermatological Association. He documented its frequency among private patients and its rarity among patients in the Venereal Disease Clinic of the Boston Dispensary. His explanation for this discrepancy was that patients in a charitable institution were less apt to complain of a trivial abnormality unless they believed it to be a manifestation of a more serious disease. He made the important observation that one of the “three” venereal diseases had existed before the appearance of herpes genitalis. His summary included the statement:
[S]ome of its most interesting and important characteristics are, its tendency to relapse, the very great frequency with which it will be found to have been preceded by the act of coitus, the fact that it rarely, if ever, is found in patients who have been perfectly free from all venereal trouble, and that it is confined to the period of youth and early manhood.
In addition, Greenough made the surprising observation that he had never seen an instance of genital herpes in a woman. Among the numerous discussants of Greenough’s paper was Louis A. Duhring (1881), president of the association, who commented in his discussion that though others had seen the disease in women, he, too, had never seen such an instance. This phase of the discussion prompted a paper 2 years later by Paul Unna of Hamburg (1883), published in an American journal. He, too, had never seen herpes genitalis in his private female patients, but cited observations made in Germany and France where medical examination of prostitutes was under police surveillance. In addition, he pointed out that among women admitted to the syphilis department of the Hamburg General Hospital, from 1878 to 1881, with admission of 1,357 to 1,459 patients annually, the incidence of herpes genitalis was 64, 126, 121, and 112 cases during the 4 years. For the same years, males admitted to the syphilis department, with admissions of 634 to 795 annually, had an incidence of herpes genitalis of 4, 9, 4, and O, respectively.
Unna (1883) summarized:
It is now evident that the conclusions arrived at by members of the American Dermatological Society are correct, in so far as the general rarity of herpes vulvae is concerned; but, on the contrary, the conclusion that women as such are therefore less susceptible of being thus affected is erroneous. Indeed, herpes progenitalis is found more frequently in women who are only distinguished by their vocation than in men. We may therefore say only this much: that women are just as susceptible to herpes as men are; there is no immunity from herpes for the female sex. On the contrary, the exciting cause that induces virile herpes is usually absent in women; but when this is present (as in puellae publicae) herpes is frequently found; for women herpes is so to say a vocational disease. (Italics added)
Unna dismissed the usual theories to account for the disease and suggested that it was a variant of
777 herpes zoster, triggered by genital irritations: Just as there are “men who are habitually attacked by herpes after each act of coition, so, too, there are prostitutes who have an eruption of herpes every time they menstruate.”
R. Bergh of Copenhagen (1890) confirmed a high incidence of herpes genitalis among prostitutes, reporting that the episodes were related to the menses in 73.4 percent of 877 women admitted to the hospital for the disease. Aware of the relationship of herpes Iabialis to bacterial infection, he was puzzled by the lack of such a relationship in herpes genitalis in spite of the not infrequent coincidence of herpes labialis and genitalis. He did not accept any relationship between herpes genitalis and venereal disease because he had seen it in a recently married woman and in youths who masturbated frequently. Therefore, he concluded the lesions were of a nervous origin, being due to congestion of the parts, as after masturbation or coitus in men and with menses in prostitutes. E. Levin (1906) reported observations on 1,584 women admitted to the venereal disease shelter in Berlin in 1898-9. There were 112 with herpes of whom 83 had genital herpes. Twenty-nine women had recurrent episodes, and thus 154 episodes were analyzed: 118 genital and 26 at other sites. Coincidence with menstruation occurred in 70 percent of the episodes.
A few years later, Prague physician O. Baum (1920) reported herpetic keratitis, following inoculation of rabbit corneas with vesicular fluid from two cases of herpes Iabialis, two of herpes genitalis (one in a recurrence), one of herpes faciei, and one each of herpes after the injection of bismuth and salvarsan. Results of such experiments with material from three cases of herpes zoster and several other vesicular skin diseases were negative. Four years later, investigators at the University of Turin, while carrying out successful experiments of inoculating blood and cerebrospinal fluid from patients having herpetic disease (or during a period between recurrences) into corneas, found instances of positive reaction among control subjects. This led to experiments with blood and cerebrospinal fluid from subjects who had not had herpetic eruptions for a long time; of 21 patients, only 3 gave negative results with both blood and spinal fluid. In 4, the spinal fluids were abnormal, and in 4 the Wassermann reaction was positive.
In 1921, B. Lipschutz successfully inoculated material from vesicles on the genitalia into the skin of human subjects. Four years later, S. Flexner and H. L. Amos (1925) demonstrated the herpes virus, and in 1934 Albert Sabin and colleagues isolated it. K. E. Schneweiss (1962) identified two strains of herpes virus by neutralization tests, a finding confirmed by W. R. Dowdle and Nahmias in 1967. The literature in subsequent years has contributed to knowledge concerning epidemiology and immunology.
R. H. Kampmeier
Bibliography
Alibert, J. L. 1832. Monographic des dermatoses. Paris.
Bateman, Thomas. 1818. A practical synopsis of cutaneous diseases. Longman.
Baum, O. 1920. Ueber die Uebertragbarkeit des Herpes Simplex auf die Kaninchenhomhaut. Dermatolo- gische Wochenschrift 70: 105—6.
Bergh, R. 1890. Ueber Herpes Menstralis. Monatshefte fur Praktische Dermatologie 10: 1—16.
Beswick, T.S.L. 1962. The origin and the use of the word herpes. Medical History 6: 214—32.
Bierman, Stanley M. 1983. A retrospective study of 375 patients with genital herpes simplex infections seen between 1973 and 1980. Cutis 31: 548-65.
Bolognese, R. J. 1976. Herpesvirus hominis type II infections in asymptomatic pregnant women. Obstetrics and Gynecology 48: 507-10.
Corey, Lawrence. 1984. Genital herpes. In Sexually transmitted diseases, ed. King K. Holmes et al. New York.
Dowdle, W. R., and A. J. Nahmias. 1967. Association of antigenic type of herpes virus hominis with site of viral recovery. Journal of Immunology 99: 974-80.
Duhring, Louis A. 1881. Discussion of Greenough paper. Archives OfDermatology 7: 29.
Flexner, S., and H. L. Amos. 1925. Contributions to the pathology of experimental encephalitis: II. Herpetic strains of encephalitogenic virus. Journal of Experimental Medicine 41: 223—43.
Greenough, F. B. 1881. Herpes progenitalis. Archives of Dermatology 7: 1-29.
Haeser, H. 1875. Lehrbuchgeschichte der Medizin und der epidemischen Krankheiten, 3 vols. Jena.
Hoeprich, P. D., ed. 1983. Infectious diseases, 3d edition. New York.
Holmes, King K., et al., eds. 1984. Sexually transmitted diseases. New York.
Kampmeier, R. H. 1984. Herpes genitalis: A clinical puzzle for two centuries. Sexually Transmitted Diseases 11: 41-5.
Legendre, F. L. 1853. M6moire sur !’herpes de la vulve. Archives Generates de Medecine 2: 171-204.
Levin, E. 1906. Ueber Herpes bein Frauen und seine Beziehungen zur Menstruation. Deutsche Medizi- nische Wochenschrift 26: 277-9; 293—6.
Lipschiitz, B. 1921. Untersuchungen iiber die Aetiologie der Krankheiten den Herpesgruppe (Herpes zoster, Herpes genitalis, Herpes febrilis). Archiv fur Dermatologic und Syphilis 136: 428—82.
Morton, R. S. 1975. Herpes genitalis. In Recent advances in sexually transmitted diseases, ed. R. S. Morton and J. R. W. Harris. London.
Nahmias1 A. J., C. A. Alford, and B. K. Sheldon. 1970. Infection of the newborn with Herpes virus hominis. Advances in Pediatrics IT 185—226.
Nahmias1 A. J.1 and Donald E. Campbell. 1983. Infections caused by herpes simplex viruses. In Infectious diseases, ed. Paul D. Hoeprich1 3d ed. Philadelphia.
Nahmias1 A. J.1 H. L. Keyserling1 and G. M. Kerrick. 1983. Herpes simplex virus. In Infectious diseases of the fetus and newborn infants, ed. J. Remington and J. O. Klein1 2d ed. Philadelphia.
Nahmias1 A. J.1 et al. 1969. Genital infection with type 2 herpes virus hominis: A commonly occurring venereal disease. British Journal of Venereal Diseases 45: 294— 8.
1981. Clinical aspects of infection with herpes simplex viruses 1 and 2. In The human herpesviruses, ed. Andre J. Nahmias1 Walter R. Dowdle1 and Raymond F. Schinazi. New York.
Preuss1 J. 1978. Biblical and Talmudic medicine (1911). New York.
Rapp1 Fred1 ed. 1984. Herpesviruses: Proceedings of a Burroughs Wellcome-UCLA Symposium, April 8—13, 1984.
Rawls1 W. E.1 et al. 1971. Genital herpes in two social groups. American Journal of Obstetrics and Gynecology 110: 682-9.
Sabin1 Albert B.1 A. Bond, and A. M. Wright. 1934. Acute ascending myelitis following a monkey bite, with isolation of a virus capable of reproducing the disease. Journal OfExperimental Medicine 59: 115—36.
Schneweiss1 K. E. 1962. Serologische Untersuchimgen zur Typendifferenzierung des Herpesvirus Hominis. Zeit- schrift fur Immunitdtsforschung und Experimentelle Therapie 124: 24-48.
Unna1 P. G. 1883. On herpes progenitalis, especially in women. Journal of Cutaneous and Venereal Diseases 1: 321-34.
US. Public Health Service. 1984. Morbidity and Mortality Weekly Report. Annual Summary, March 33: 90.
Willan1 Robert. 1808. On Cutaneous Diseases, Vol. 1. London.
More on the topic 64 Herpes Simplex:
- 64 Herpes Simplex
- Contents
- Kiple Kenneth F. (Editor). The Cambridge World History of Human Disease. Cambridge University Press,1993. — 1200 p., 1993